Medicaid Unwinding’s Impact on Enrollment Estimates
Medicaid enrollment rose across the country toward the end of state fiscal year (FY) 2020 through FY 2023. Federal legislation tied to the Public Health Emergency (PHE) incentivized states to maintain eligibility for Medicaid enrollees during the COVID-19 pandemic by increasing federal funding for Medicaid programs. In response, Kansas, and all other states, delayed action on annual reviews, ensuring continuous Medicaid coverage during this time period. Continuous coverage significantly reduced disenrollment and “churn” (disruption in coverage) during the PHE. In April 2023, the continuous coverage provision for Medicaid ended, and states were given 12 months to redetermine eligibility for those on Medicaid. This process, often referred to as “unwinding,” is underway through April 2024.
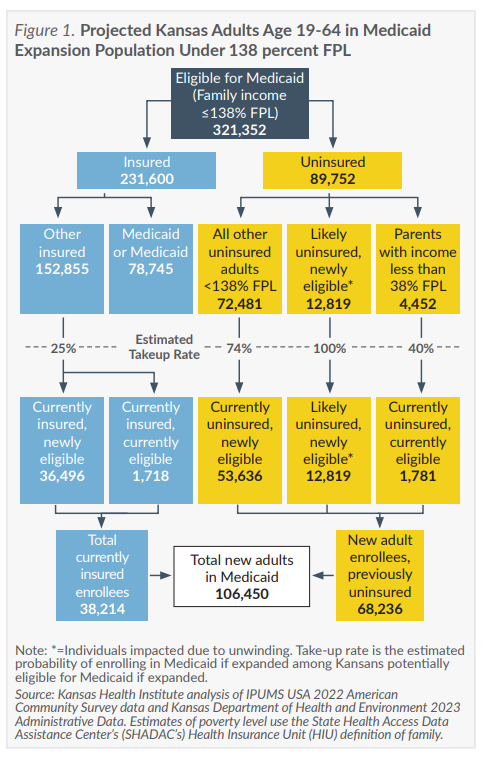
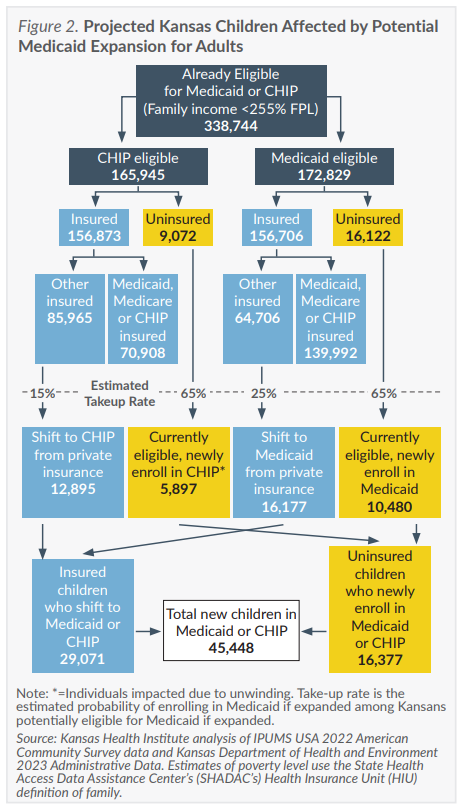
The updated expansion enrollment estimates account for the effect of unwinding on adults and children who may have lost eligibility at the end of the continuous coverage period. The estimate includes 12,819 adults disenrolled from Medicaid who would likely enroll under expansion, as well as 5,913 children who lost eligibility but would be more likely to re-enroll in KanCare if Medicaid were expanded.
A Closer Look at the Medicaid Expansion Population: Selected Characteristics
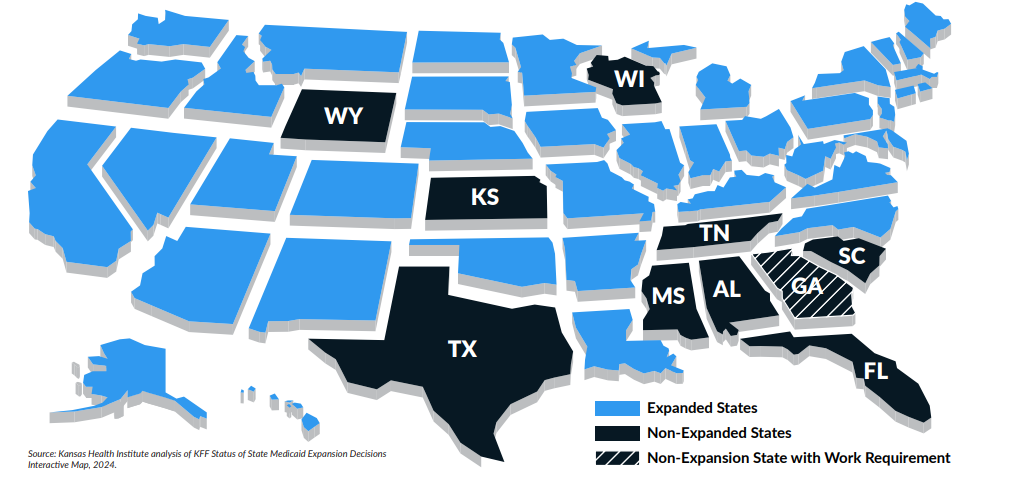
Gov. Kelly’s proposed Medicaid expansion includes a work requirement with some exemptions for full-time students, full-time caregivers, veterans, individuals with disabilities, volunteers, individuals experiencing homelessness, former foster youth under age 22 and those experiencing hardship as determined by the Secretary of KDHE for adults in the expansion population.
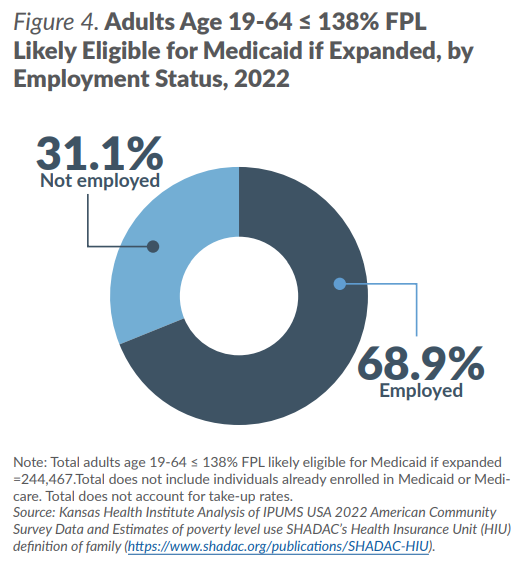
The accompanying insert includes analysis for likely eligible Kansas adults age 19-64 as well as for Kansas adults age 19-64 in the expansion population who are not employed (31.1 percent), but who may meet some exemptions to the proposed work requirement.
Costs
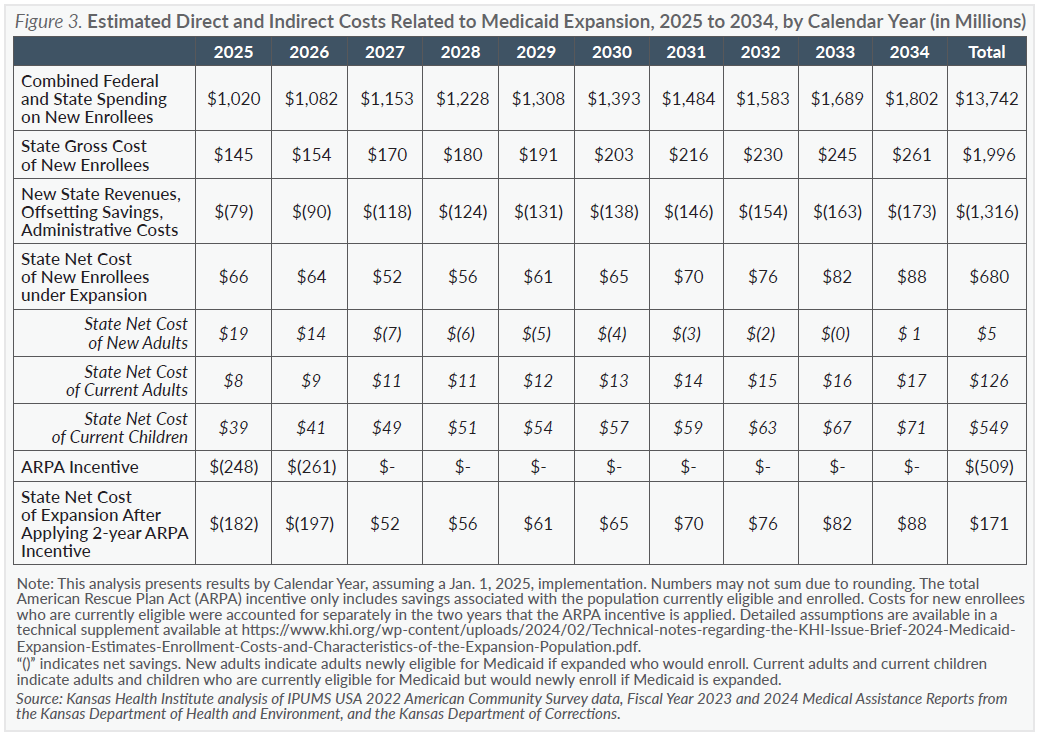
This estimate assumes expansion would be implemented on Jan. 1, 2025. The estimated net cost to the state of $171 million over 10 years includes new revenues, savings from adults who would enroll in the new expansion group (with a federal match rate of 90 percent) rather than another eligibility group with a less-favorable match rate (regular match rate of around 60 percent), additional administrative costs from new enrollment, and a two-year 5-percentage point bump in the federal match rate for traditional Medicaid populations enacted in the American Rescue Plan Act (ARPA) in 2021 as an incentive to states to newly expand their programs. The ARPA incentive remains available to states that have not yet expanded Medicaid. For Kansas, the incentive would be worth an estimated $509 million over two full years.
The resulting estimated costs are presented in Figure 3, page 4. Over 10 years, estimated total costs including federal and state spending would increase. However, if Medicaid were expanded to low-income adults under the terms of the ACA, it would offset the equivalent of approximately eight years worth of net state expansion costs. Further, net state costs for new adult enrollees are estimated to be nearly revenue neutral over a 10-year period ($5 million).
Estimated new annual revenues associated with new KanCare enrollees include managed care privilege fees, increased drug rebates collected by the state, additional CHIP premiums collected and a hospital surchage ($233 per expansion enrollee in the aggregate) beginning in 2027, as outlined in Gov. Kelly’s expansion proposal.
The estimated savings each year from expansion is associated primarily with enrollees who otherwise may have been in different eligibility groups, such as women who would become pregnant while already enrolled in the expansion group as well as those in the expansion group who would have qualified as Medically Needy, who would have enrolled in the entirely state-funded MediKan program or who may otherwise have been eligible through Supplemental Security Income. State savings also are estimated to account for inmates who could be eligible for Medicaid in the case of a hospital admission longer than one day.
The estimated state net costs do not include the projected effects on the workforce or the overall state economy. A February 2021 analysis by John Leatherman, a professor in the Department of Agricultural Economics at Kansas State University, suggested that expanding Medicaid would increase economic output, thus generating each year additional state tax revenue of between 3.1 percent and 3.9 percent and local tax revenue of between 2.3 percent and 2.9 percent of the federal cost of new enrollees. This cost estimate does not assume the state would reduce funding for other programs that currently provide services for uninsured Kansans, including safety net clinics and community mental health centers.