Introduction
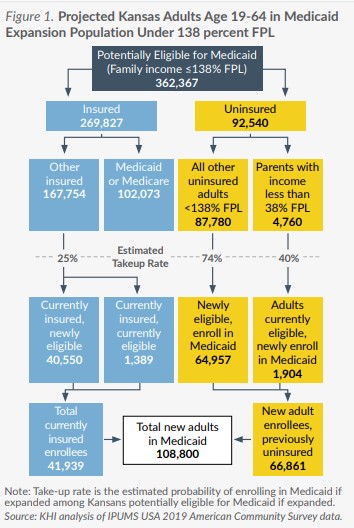
An estimated 87,780 uninsured Kansans who could be eligible for Medicaid if expanded under the terms of the Affordable Care Act (ACA) currently make too much to qualify for Medicaid and too little to qualify for subsidized coverage on the ACA health insurance marketplace, falling into the so-called “Medicaid coverage gap.” Medicaid expansion would allow these uninsured Kansans to enroll in KanCare, the state program that provides Medicaid coverage. A new federal incentive has changed the financial equation for states that newly expand Medicaid coverage, but it is unclear whether this financial incentive will change the policy preferences of a majority of Kansas lawmakers.
This issue brief provides an updated estimate of the impact that expanding Medicaid coverage would have on KanCare enrollment and expenditures using the best available data on population, costs and savings. Expanding KanCare to all adults age 19-64 with family income at or below 138 percent of the federal poverty level (FPL, $38,295 per year for a family of four in 2022) has been a perennial issue for the Kansas Legislature since the U.S. Supreme Court made Medicaid expansion optional for states in 2012. Currently, Kansas adults are eligible for Medicaid if they are age 65 or older, blind or have a disability and meet income and resource requirements, or if they are a parent or guardian with family income below 38 percent FPL ($10,545 per year for a family of four in 2022).
In February 2022, Governor Laura Kelly and expansion supporters in the Legislature introduced new legislation, House Bill (HB) 2675 and Senate Bill (SB) 472, to expand KanCare effective January 1, 2023. Unlike expansion legislation introduced in 2021, which paired expansion with revenue from the legalization of medical cannabis, the 2022 bills are focused on expansion alone and hope to capitalize on a new federal incentive created by the American Rescue Plan Act of 2021 (ARPA), which would provide savings to the state that are similar to the initial incentive offered in the first six years of the ACA but would provide those savings over two years. In announcing HB 2675 and SB 472, the Governor noted that the state estimates net savings to the state general fund in the first fiscal year, which she proposed reallocating for a one-time investment in housing, child care and workforce development programs.
Federal Medicaid Expansion Financial Incentive
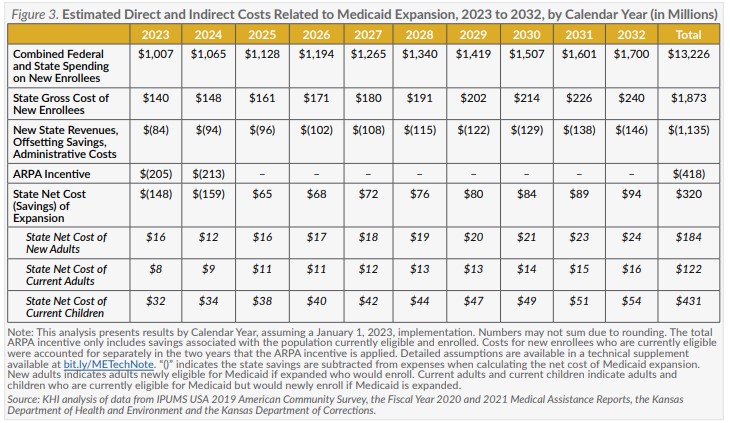
ARPA provides states that newly expand their Medicaid programs a five percentage point increase in the Federal Medical Assistance Percentage (FMAP) applied to spending on most currently eligible Medicaid enrollees for two years (eight quarters) after expansion. Adults newly eligible because of expansion would receive the standard 90 percent FMAP for expansion enrollees. In Kansas, the federal share of spending would effectively increase from 60 cents to 65 cents of each dollar spent on KanCare members currently enrolled in the qualifying groups. The KanCare program spends around $4 billion a year on benefits for those who would qualify for the increased FMAP resulting in about $200 million per year in savings if Medicaid were expanded.
Enrollment in Medicaid and the Children’s Health Insurance Program (CHIP) in Kansas has increased 21 percent during the pandemic due to changes in the economy and administrative policies adopted to prevent beneficiaries from being disenrolled. Those policies were required by the Families First Coronavirus Response Act as a condition for states to obtain a temporary 6.2 percentage point increase in the FMAP during the federal COVID-19 public health emergency (PHE). Barring new federal legislation, the 6.2 percentage point increase in the FMAP will last through the end of the quarter in which the federal PHE ends (the current declaration expires July 15, 2022).
This estimate assumes all beneficiaries who would no longer be eligible after the PHE ends would be disenrolled before January 1, 2023. After adjusting for spending and enrollment trends before the PHE, the ARPA incentive was estimated to be $205 million in 2023 and $213 million in 2024. The cost of expansion would be lower if the PHE were still in effect.
While other policy changes that ultimately were adopted during the 2022 legislative session — such as extending Medicaid benefits for pregnant women to one year post-partum — may impact the number of new enrollees and cost, the end of the 6.2 percentage point increase is the only policy change other than Medicaid expansion assumed in this estimate.
Enrollment Estimate
As in previous KHI estimates, the estimate in this brief represents all those who are expected to enroll if Medicaid is expanded. This assessment differs from other estimates of Medicaid expansion enrollment, including state fiscal notes, because it includes potential indirect effects of expansion, such as currently eligible children and adults who might newly enroll in an expanded Medicaid program.