Kansas will soon be bordered on all sides by states that have expanded Medicaid coverage to low-income adults under the terms of the Affordable Care Act.
Using data from before the COVID-19 pandemic, a total of 126,000 Kansans, including nearly 88,000 adults and 39,000 children, are estimated to newly enroll in KanCare if Medicaid were to be expanded in January 2022.
While the estimated new enrollment represents an increase of approximately 31 percent from recent KanCare enrollment, expansion would be estimated to increase total state KanCare spending by just 2.7 percent per year on average over a 10-year period, compared to projections based on the pre-pandemic trend.
The estimate differs from state fiscal notes and other estimates because it includes the indirect effect of expansion on enrollment of children and currently eligible adults.
COVID-19 has increased Medicaid enrollment in all states, including those states that have not expanded Medicaid, as federal pandemic relief encouraged states to adopt administrative policies to prevent current beneficiaries from being disenrolled.
The effects of COVID-19 on expansion enrollment beginning in January 2022 are difficult to project, but if the economic effects of the pandemic persist, Medicaid expansion would offer an option for insurance coverage for those who remain unemployed.
Introduction
With the passage of ballot initiatives in 2020, Missouri and Oklahoma joined Nebraska and Colorado to completely surround Kansas with states that have already expanded or will soon expand Medicaid coverage to low-income adults under the terms of the Affordable Care Act (ACA). That changing landscape, combined with a new federal administration and the lingering effects of the COVID-19 pandemic, is likely to influence debate over Medicaid expansion in Kansas in 2021.
Medicaid and the Children’s Health Insurance Program (CHIP) are known together in Kansas as KanCare. The ACA expansion opportunity allows states to expand Medicaid eligibility to adults age 19-64 with income up to 138 percent of the federal poverty level (FPL, $36,570 for a family of four in 2021). Kansas is now one of 12 states that have not adopted expansion.
This issue brief updates previous Kansas Health Institute (KHI) estimates of the impact a potential expansion of Medicaid would have on KanCare enrollment and costs, using a methodology consistent with previous estimates. The brief also discusses potential effects of the COVID-19 pandemic on the expansion population.
In early 2020, an agreement between Governor Laura Kelly and former Senate Majority Leader Jim Denning led to the introduction of expansion legislation that was cosponsored by 22 of the 40 members of the Senate. However, the legislation stalled in committee and, in a session cut short by COVID-19, expansion did not advance. On February 1, 2021, Governor Laura Kelly announced a new effort to expand KanCare. The proposal builds on previous legislation to expand the program but creates a new funding mechanism for the state share of expansion with revenue from the legalization of medical marijuana.
This analysis uses the latest available population information as well as updated costs and revenues to project that Medicaid expansion would result in the enrollment of approximately 126,000 additional Kansans — a 31 percent increase from the average monthly enrollment over the last three fiscal years. The increase in enrollment would be expected to result in net cost to the state in the first full calendar year (2022) of $14.1 million for newly eligible adults, $10.9 million for currently eligible but newly enrolled adults, and $31.0 million for newly enrolled children. Over a ten-year period, expansion would be estimated to increase total state Medicaid spending by an average of 2.7 percent per year compared to projections made from pre-COVID-19 trends.
Enrollment Estimate
As in previous KHI estimates, the estimate in this brief represents all those who are expected to enroll if Medicaid is expanded. This assessment differs from other estimates of Medicaid expansion enrollment, including state fiscal notes, because it includes potential indirect effects of expansion, such as currently eligible children and adults who might newly enroll in an expanded Medicaid program. The analysis uses U.S. Census Bureau data from the 2019 American Community Survey (ACS) to estimate the number and insurance status of the population that would enroll in Medicaid if it were expanded.
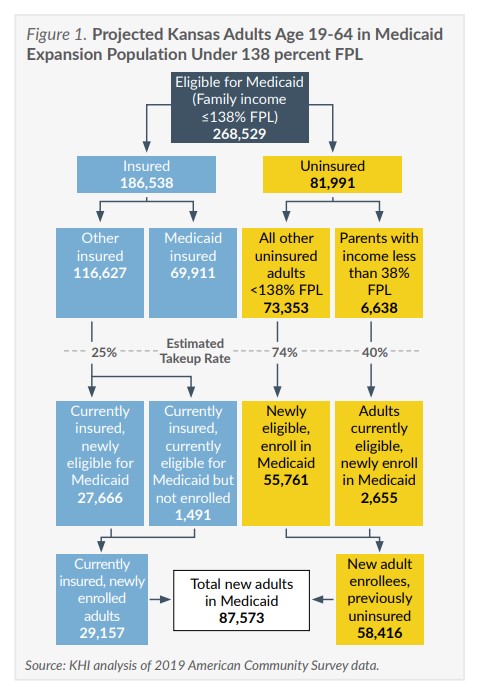
The estimate of 126,098 additional enrollees includes 87,573 adults and 38,525 children. Of the 87,573 new adult enrollees (Figure 1), 55,761 are newly eligible adults who are currently uninsured, 2,655 are adults who are currently eligible but uninsured, and 29,157 are adults who would be expected to switch from another insurance source to KanCare. This estimate does not account for the potential of increased enrollment due to higher rates of unemployment or the policy response to the COVID-19 pandemic.
This brief also considers some adult enrollment in KanCare that could shift to the expansion group, which is estimated to reduce state costs as discussed in the next section. Approximately 9,300 current KanCare members who might otherwise have enrolled in pre-expansion eligibility categories could instead become eligible in the new expansion group. That effect would increase the adult enrollment in the expansion group but not total enrollment, so the group is not included among the 126,000 estimated “new” enrollees.
Expanding Medicaid would not change the eligibility levels for children, but it is assumed that more currently eligible children who are not enrolled would enroll in KanCare as outreach efforts following expansion reached more people, particularly if their parents were to newly enroll. The estimate of 38,525 newly enrolled children (Figure 2) includes 17,524 currently uninsured children and 21,001 children whose coverage would shift to KanCare from other coverage.
Cost
This estimate assumes expansion would be implemented on January 1, 2022. The total gross costs in this estimate are lower than in previous KHI estimates primarily because the expected number of new enrollees declined. This is partly because of a decrease in the number of low-income adults who were otherwise insured and fewer uninsured adults and children in the 2019 ACS. Actual KanCare per capita costs, which are the basis for the per enrollee cost in the analysis, have increased. The assumed take-up rates and projected annual increase for expansion-related costs are the same as estimated last year.
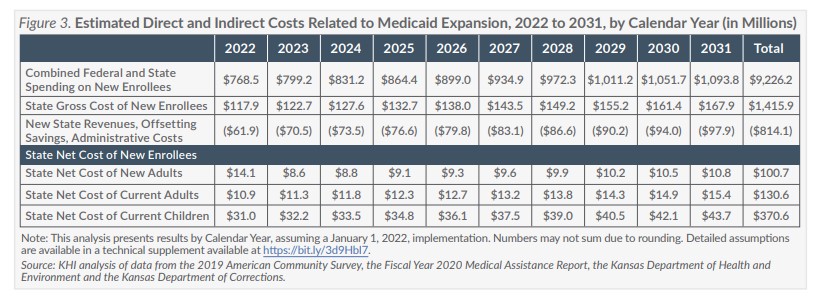
The estimated net cost to the state also declined compared to the estimate from last year because fewer adults and children who are currently eligible are expected to newly enroll. The estimated net cost to the state includes estimated new revenues, savings from adults who would enroll in the new expansion group (with a federal match rate of 90 percent) rather than another eligibility group with a less favorable match rate (regular match rate of 60 percent), and additional administrative costs from new enrollment. The resulting estimated costs are presented in Figure 3.
Estimated new annual revenues associated with new KanCare enrollees include managed care privilege fees, increased drug rebates collected by the state, and additional CHIP premiums collected. The estimated savings each year from expansion are associated primarily with enrollees who are currently eligible, but would enroll in Medicaid expansion rather than another eligibility group. Those enrollees include some women who would become pregnant while already enrolled in the expansion group, nearly all adults who might have enrolled in the entirely state funded MediKan program, and some adults who would have qualified as Medically Needy or who may otherwise have been eligible through Supplemental Security Income. State savings are also estimated to account for inmates who could be eligible for Medicaid in the case of a hospital admission longer than one day.
The most recent experience was used to estimate the savings associated with enrolling those who are currently eligible because of medical need or pregnancy in the expansion group and the increased administrative cost associated with expansion. The assumptions of savings, revenue and administrative costs are otherwise the same as estimated last year. The details of each assumption are provided in a technical supplement available online.
The estimated state net costs do not include the projected effects on the workforce or the overall state economy. Previous analysis by John Leatherman, a professor in the Department of Agricultural Economics at Kansas State University, suggested that expanding Medicaid would increase economic output, thus generating each year additional state tax revenue of between 2.9 percent and 3.6 percent and local tax revenue of between 2.4 percent and 3.0 percent of the federal cost of new enrollees. This cost estimate does not assume the state would reduce funding for other programs that currently provide services for uninsured Kansans, including safety net clinics and community mental health centers.
In addition, like the enrollment estimate, the estimated cost does not account for the impact of the COVID-19 pandemic or the related policy response.
Expansion and COVID-19
While the estimates of Medicaid expansion enrollment and costs in this brief use data that predate COVID-19, the pandemic has affected Medicaid policy in Kansas and across the country in ways that may outlast the pandemic itself.
Enrollment in Medicaid and CHIP has increased during the pandemic in both expansion and non-expansion states, particularly as states adopted administrative policies to prevent current beneficiaries from being disenrolled. Those policies, which were required by the Families First Coronavirus Response Act as a condition for states to obtain a temporary increase of 6.2 percentage points to the federal match rate during the pandemic, combined with increased unemployment led to a 9.4 percent increase in nationwide Medicaid and CHIP enrollment between February and September 2020.
Increases in enrollment varied across states but increased in all. Among the six states with the largest percentage increase in enrollment (over 15 percent), three had expanded Medicaid (Kentucky, Nevada and Utah), and three had not (Missouri, Oklahoma and Wyoming). In Kansas, the increase in Medicaid and CHIP enrollment was 10.2 percent (about 38,600) between February and September 2020, and enrollment continued to increase through the fall.
Researchers have noted that Medicaid enrollment lags changes in unemployment, so the COVID-19 effect on enrollment may linger. For example, wages before job loss, combined with unemployment benefits, may have kept annual income for some above the poverty level, making them eligible for subsidies on the federally facilitated insurance marketplace. However, as people facing extended unemployment exhaust those benefits, it will affect both enrollment and the number of people who fall in the coverage gap — those who make too little to qualify for marketplace subsidies (less than 100 percent FPL) but who do not qualify for Medicaid in non-expansion states such as Kansas.
Unemployed workers who may have been eligible for marketplace subsidies in 2020 because of unemployment benefits may fall into the coverage gap when benefits expire. A study published in May 2020, prior to the extension of unemployment benefits passed by Congress in December, estimated that as many as 52,000 Kansans who could become uninsured because of job loss would fall into the coverage gap by January 2021. Many of the Kansans in that group would not have been among the 126,000 new enrollees projected if Kansas were to expand Medicaid starting in 2022, but if the economic effects of the pandemic persist, Medicaid expansion could offer coverage for those remaining unemployed.
The temporary 6.2 percentage point increase in the regular federal match rate (currently about 60 percent in Kansas), while not applicable to the 90 percent federal match rate for the expansion population, has shielded states from the bulk of the financial effect of COVID-19 on Medicaid budgets. The increased match is slated to last through the end of the quarter in which the COVID-19 public health emergency ends.
Conclusion
The effects of COVID-19 may echo through Medicaid long past the end of the pandemic, but its effect on the Medicaid expansion debate in Kansas is uncertain. Advocates for the expansion of KanCare note that the COVID-19 pandemic highlights the critical value of health insurance coverage, particularly for lower-income Kansans. facing unemployment or working in front-line jobs. The pandemic also worsened financial stress on hospitals and other health care providers that could be partially offset by patients newly covered by an expanded KanCare program.
Access additional publications in the Documents & Downloads section.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.