

Hill to the Heartland: Federal Health Policy Briefing is a product series providing regular updates on federal health policy discussions. Sign up here to receive these summaries and more, and also follow KHI on Facebook, Twitter, LinkedIn and Instagram.
Potential Impacts of Federal Policy Decisions on Medicaid and CHIP in Kansas
Hill to the Heartland: Federal Health Policy Briefing
16 Min Read
Mar 12, 2025
By
Sheena L. Schmidt, M.P.P., Emma Uridge, M.P.H., Kaci Cink, M.P.H., Shelby C. Rowell, M.P.A.,Alexa Heseltine

The Kansas Health Institute (KHI) is closely monitoring federal health policy developments to assess their potential impact on Kansans. Through ongoing analysis and tracking of legislative and administrative proposals, KHI is committed to providing insights into how potential changes at the federal level could affect key issues related to health insurance coverage, public health, and funding and health care access for those covered by Medicaid and the Children’s Health Insurance Program (CHIP) in Kansas.
Congress is currently considering changes to Medicaid that could have significant implications for state programs, including KanCare. Medicaid and CHIP, otherwise known as KanCare in Kansas, provide coverage for health services and long-term care to approximately 440,000 eligible low-income dependent children, parents, pregnant women, people with disabilities and older adults, as well as some individuals with specific health conditions.
Federal policy decisions play a crucial role in shaping Medicaid’s funding, eligibility and coverage, making it essential to understand how proposed changes might impact Kansans. The policy options outlined below are under consideration and may not be implemented by Congress. However, they provide insights into potential changes and may have significant implications for state budgets, Medicaid beneficiaries and health care providers. With a Republican majority in both the House and Senate, lawmakers are negotiating a budget resolution that, when agreed to by both chambers, will lay the groundwork for major fiscal policy shifts. The House recently passed a resolution that sets the stage for $4.5 trillion in tax cuts alongside reductions in federal spending ranging from $1.5 to $2 trillion over the next decade. However, the Senate has its own budget resolution, focusing on increased funding for border security, energy development and military defense, with tax policy to come in a second phase of legislation later in the year.
As Congress enters the budget reconciliation process, the details of these potential changes will be negotiated, shaping the future of Medicaid and other critical programs.
Quick Facts:
- Medicaid provides comprehensive health coverage and long-term care to approximately 83 million Americans. It covers approximately 4 in 10 births in the United States.
- Medicaid is traditionally the third-largest domestic program in the federal budget, behind only Medicare and Social Security. In Kansas, Medicaid ranks second in spending (state and general funds) behind only K-12 education.
- The Medicaid program is jointly funded by the federal government and the states. By law, every state receives at least a 50 percent match in federal dollars. The match rate, known as the Federal Medical Assistance Percentage (FMAP), varies by state.
- Medicaid: In fiscal year (FY) 2025, the FMAP in Kansas is 61.87 percent, meaning that for every $1 that Kansas spends on Medicaid, the federal government contributes $1.62.
- CHIP: The FY 2025 FMAP for CHIP is 73.31 percent in Kansas.
- Medicaid in Kansas is administered by the Kansas Department of Health and Environment (KDHE) and the Kansas Department for Aging and Disability Services. Kansas contracts with managed care organizations (MCOs) that provide health coverage for most Medicaid beneficiaries in Kansas.
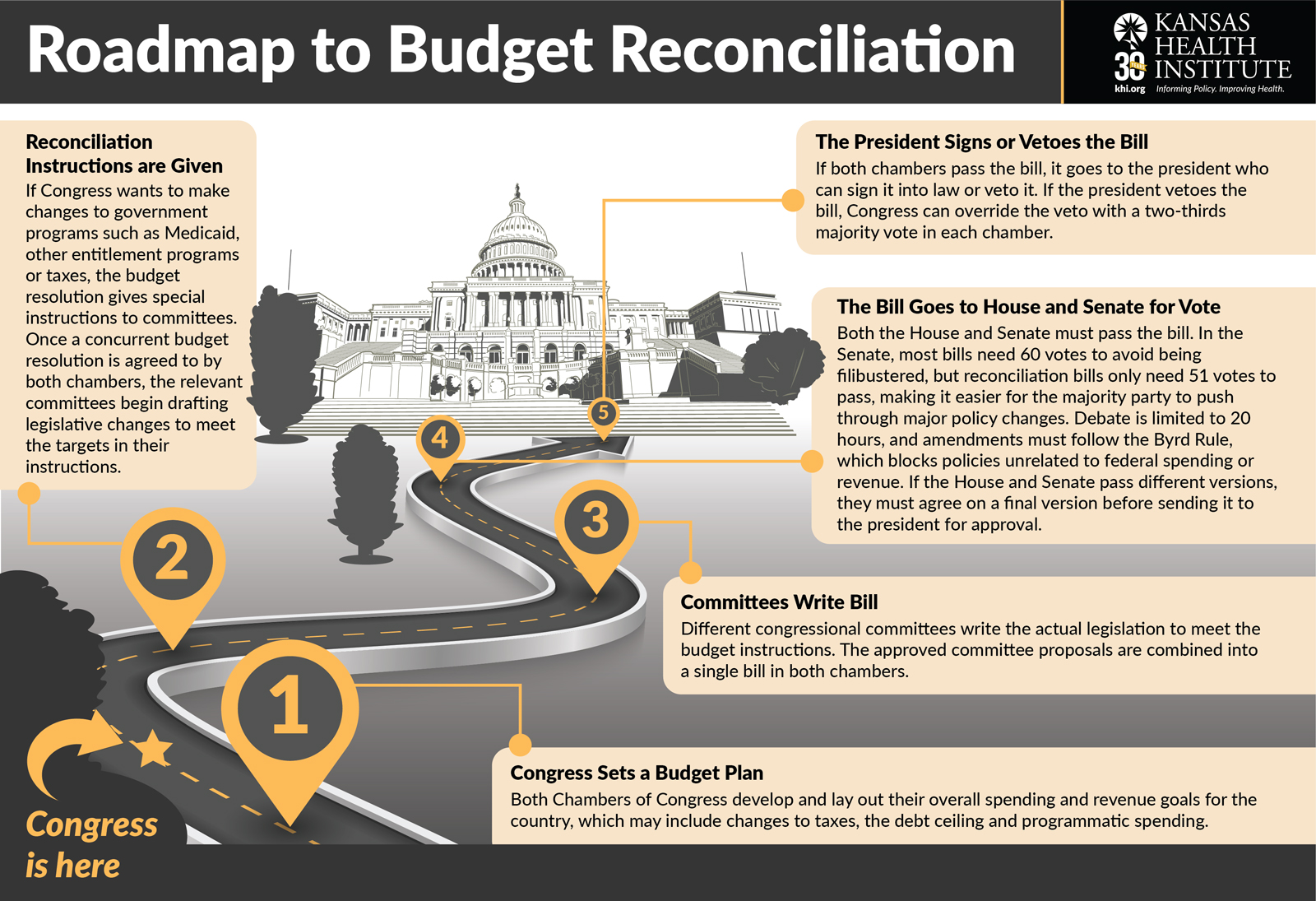
Unpacking the Congressional Budget Reconciliation Process
The budget reconciliation process is used for budget-related issues directly related to revenues and mandatory spending (also referred to as entitlement spending). The process allows Congress to pass certain budget-related laws more quickly than usual. The budget reconciliation process helps lawmakers change spending, taxes or federal debt without needing as many votes as other bills. It cannot be filibustered in the Senate, which means the minority party has less power to block it. The steps of the process are outlined in Figure 1.
Current Status
The House and Senate have both made progress by passing separate budget resolutions, but before they can advance to the next step, both chambers must agree on a resolution that can pass both the House and Senate.
The House budget resolution, which was passed on Feb. 25, calls for a reduction of $1.5‒$2 trillion in spending over ten years. The House resolution includes instruction for the House Energy and Commerce Committee — which oversees health care programs, including Medicaid and CHIP, the Affordable Care Act (ACA) programs, Medicare, substance use and mental health programs, and several public health agencies — to cut $880 billion in spending over 10 years. Because Medicaid is one of the largest federal programs in the budget, the House Energy and Commerce Committee would likely have to make cuts to Medicaid to meet its spending reduction target. With some congressional members expressing hesitancy to cut from the Medicaid budget, it is unclear how Congress will move forward. According to the Congressional Budget Office (CBO), the House Energy and Commerce Committee would not be able to meet its budget target without cutting Medicaid or Medicare. When Medicare is set aside, the total funding under the committee’s jurisdiction is $8.8 trillion over 10 years, with Medicaid accounting for $8.2 trillion (93 percent). When Medicare, Medicaid and CHIP are excluded, the committee oversees a total of $381 billion in spending over 10 years. Put another way, even if all other programs under the Committee’s jurisdiction were eliminated, it would still necessitate cuts of approximately $500 billion to Medicare, Medicaid or CHIP to reach the $880 billion target.
The Senate favors a two-step approach with its budget resolution, which was passed on Feb. 21 and directs relevant committees to spend $342 billion on immigration enforcement, energy production and the military in one bill. Because the Senate plan was to go through a second process later in the year to address tax policy, the current Senate version of the budget resolution has a much smaller instruction for savings to the Senate Finance Committee, which has jurisdiction over Medicaid. The instruction would require the Committee to cut at least $1 billion from programs in its jurisdiction over 10 years.
Senate leadership has indicated plans to take up and amend the House version of the budget resolution, but the timing is unclear. Ultimately, the House and Senate must pass the same concurrent resolution to proceed with the budget reconciliation process, meaning both chambers will have to agree on the approach.
How the Budget Reconciliation Process Could Impact Medicaid
The process is still in its early stages, as the House and Senate have not yet agreed on a budget resolution. In the meantime, policymakers and stakeholders in Kansas can review some of the ways Congress might find savings from the Medicaid program if cuts are required. The following sections outline these options and their potential impact to Kansas if implemented. A menu of budget options that was circulating on Capitol Hill and that was published by media outlets in January included changes that could affect Medicaid. These options include changing Medicaid’s funding structure, modifying eligibility requirements, changing funding for Medicaid expansion or rescinding certain existing Medicaid rules.
1. Change How Medicaid is Funded
The federal government currently provides a percentage of Medicaid costs, with states paying the remaining share through various funding mechanisms, including taxes, State General Fund (SGF) revenue and other sources. Medicaid will likely make up a portion of the $880 billion cut outlined in the House Budget Resolution. Consideration could be given to restructuring Medicaid funding mechanisms to decrease federal spending obligations.
Convert Medicaid Funding from Uncapped Spending to a Per Capita Cap
Under the current structure, states receive at least a 50 percent FMAP (federal match rate) for allowable Medicaid expenses, without a limit. Kansas currently receives a higher FMAP rate (61.87 percent for Medicaid and 73.31 percent for CHIP) than some other states, ranking 24th for Medicaid and CHIP FMAP among the 50 states and Washington D.C. If federal funding were subject to per capita caps, the total amount each state could receive in matching funds could not exceed a predefined amount per enrollee, subject to a limited annual growth rate.
Potential Impacts:
- The full extent of the impact of a per capita cap on Kansas would largely depend on the intent and design of this funding structure (for example, what year would be used as a baseline and what rate would be used to limit cost growth), but the state would need to pay health care costs that exceed the federal cap.
- To close the funding gap between capped funding and actual health care costs, Kansas and other states may be required to reallocate state resources from the State General Fund or find other revenue sources to pay for its share of the costs. One analysis indicates the effect of a per capita cap on the Kansas budget, if eligibility levels were maintained and estimated cost growth continued, could be $2.5 billion over 10 years.
The concept of a per capita cap has been proposed before, including in 2017 during attempts to repeal and replace the Affordable Care Act, but has not been adopted. Further, House Speaker Mike Johnson indicated on Feb. 26 in an interview that a per capita cap was not on the table.
Limit Use of Medicaid Provider Taxes to Fund the State Share of Medicaid Costs
States use a variety of funding sources to finance the state portion of Medicaid spending, with provider taxes being an integral component to both generate additional funds to support Medicaid services and improve access to care. In FY 2025, 49 states, including Kansas, and the District of Columbia used at least one provider tax to finance their Medicaid program, indicating the funding mechanism’s widespread utilization. The federal House Budget Blueprint calls for reducing the provider tax rate to 3 percent.
Currently, Kansas assesses provider taxes on the following entities as part of its financing strategy:
- Hospitals (3 percent). Last year, the Kansas Legislature required KDHE to request approval from the Centers for Medicare and Medicaid Services (CMS) to raise the Health Care Access Improvement Program (HCAIP) provider tax for hospital inpatient and outpatient services to at least 5 percent but not more than 6 percent, which is the maximum allowable rate permitted under federal law for provider taxes used to finance Medicaid. KDHE was required to submit a tax waiver request to CMS, and it is currently pending approval.
- Nursing facilities ($4,908 per licensed bed in facilities annually)
- Continuing care retirement communities, facilities with no more than 45 skilled nursing beds, and high Medicaid volume facilities providing multiple levels of care ($818 per bed)
Kansas also charges a privilege fee of 5.77 percent to health maintenance organizations, including KanCare managed care organizations, that provides revenue for the Medicaid program. CMS does not consider premium taxes or privilege fees to be a provider tax.
Potential Impacts
- Provider taxes generate matching federal Medicaid funds, which are then redistributed to enhance reimbursement rates for hospitals, physicians, nursing facilities, and home health care providers throughout the state.
- Limiting this financing mechanism could require Kansas to find alternative sources of revenue to fund more of its share of Medicaid costs, impacting other budget priorities.
Lower the FMAP Rate for Administrative Costs
Under current law, the matching rate for states’ administrative costs related to Medicaid is generally set at 50 percent. However, certain functions qualify for a higher FMAP ranging from 75 percent to 100 percent, including upgrades to eligibility systems (e.g., the Kansas Eligibility Enforcement System), operation of surveying and certifying nursing facilities, operation of state Medicaid fraud control units, implementation and operation of immigrant status verification systems, administration of family planning services, and other functions. This proposed change would lower the FMAP for all administrative costs to 50 percent.
Potential Impacts:
- For administrative costs, a reduction of enhanced FMAP could result in significant challenges for state budgets. For example, based on data from FY 2023, if the federal matching rate were reduced to 50 percent for all administrative costs, it would impact the state budget by $31 million.
2. Institute Work Requirements
Changing Medicaid eligibility requirements also may be considered under reconciliation, which includes implementing mandatory work requirements to receive Medicaid benefits. This could potentially reduce the number of individuals who qualify for coverage. While there is no current language that indicates the specific requirements for this policy, proponents of this policy are likely referring to a work reporting requirement included in the House debt-ceiling bill passed in 2023 which would require adult enrollees ages 19‒55 to work or participate in other qualifying activities such as community service or job training for at least 80 hours per month. Under that proposal, all adult Medicaid recipients except for individuals with disabilities or who are pregnant, students or caregivers would have been required to demonstrate their employment status. A recent KFF analysis of the U.S. Census Bureau’s Current Population Survey found that nearly two-thirds of non-elderly adults with Medicaid coverage were working full or part time. Reasons for not working included school attendance, illness, disability or caregiving.
Potential Impacts:
- Enrollees of Medicaid may be at risk of disenrollment despite meeting work requirements due to reporting barriers and administrative complexities. For example, Arkansas’ work requirement led to more than 18,000 people losing coverage due to noncompliance in reporting. The requirements were in effect from June 2018 through March 2019.
- Administrative complexities in verifying work requirement compliance may put a strain on state resources and lead to higher administrative costs, which could offset potential cost savings from decreased enrollment. Earlier this year, Georgia adjusted verification of employment from a monthly basis to an annual basis due to administrative challenges.
3. Change Funding for Medicaid Expansion
Congress also is considering modifications to how Medicaid expansion is funded, which could significantly impact states that have expanded or are considering expanding Medicaid coverage. Proposals include reducing the enhanced federal match rate for the expansion population and removing financial incentives for non-expansion states, which could result in more costs being shifted to states that have expanded Medicaid or choose to expand in the future. Kansas is one of 10 states that has not expanded Medicaid. Governor Laura Kelly has proposed several expansion plans during her tenure. The most recent legislation, called the Healthcare Access for Working Kansans Act, or HAWK Act, proposes to expand Medicaid to individuals making less than 138 percent of the federal poverty level (FPL, $21,597 for an individual in 2025) and includes a work requirement of at least 20 hours per week with exceptions for full-time students, parents or guardians of dependents, individuals with disabilities or those applying for Supplemental Security Income (SSI) / Social Security Disability Insurance (SSDI), veterans, homeless individuals, and volunteers working at least 20 hours per week.
According to KHI analysis of 2022 IPUMS data from the U.S. Census Bureau, an estimated nearly 7 in 10 (68.9 percent) Kansans would meet the requirement of working at least 20 hours per week under the HAWK Act, and many others would meet one or more exceptions outlined above.
Eliminate Enhanced FMAP for Medicaid Expansion
In many other states, Medicaid also covers eligible adults without children up to 138 percent FPL. Kansas is one of 10 states that has not expanded Medicaid. Thus, adults age 19‒64 without children are not eligible for Medicaid in Kansas even if their income is $0, unless they qualify because of pregnancy, disabilities or specific health conditions. Under current law, the federal government covers 90 percent of the cost for the expansion population on a permanent basis, with states being responsible for covering the remaining 10 percent of costs. Proposals to reduce the enhanced FMAP for Medicaid Expansion would likely reduce the federal government’s share to each state’s normal match rate.
Potential Impacts:
- For non-expansion states like Kansas, without the increased FMAP, it would be less financially viable to pursue Medicaid expansion.
- Based on KHI analysis last year, if the federal match rate for expansion enrollees was reduced from 90 percent to Kansas’ current match rate of 61.87 percent in FY 2025, the state net cost of newly eligible adult enrollees would increase by approximately $3 billion over a ten-year period, if the American Rescue Plan Act (ARPA) incentive remained (see below).
- Current expansion states would need to adjust their budgets to take on potentially a much larger share of expansion costs. Some may roll back expansion due to provisions that require them to do so if the 90 percent federal match rate goes away. The HAWK Act also includes such a provision.
Eliminate the Additional Incentive for States to Implement Medicaid Expansion
Under current law, if remaining non-expansion states were to adopt Medicaid expansion, they would receive an additional five percentage point increase in their regular FMAP for two years. However, if Congress eliminates this provision from ARPA, non-expansion states would lose this financial incentive, which has been a major driver in other states, such as North Carolina’s decision to expand Medicaid.
Potential Impacts:
- According to KHI’s 2024 analysis, Kansas would have received $509 million for choosing to expand Medicaid, which would have covered approximately eight years of net state expansion costs.
- Without the funding incentive, states like Kansas may see slower, or stalled, expansion decisions.
4. Repeal or Rescind CMS Rules
Congress also is considering key rule changes designed to reduce the share of Medicaid costs. Potential options include:
- Rescinding or repealing a rule finalized in May 2024 focused on increasing staff level requirements for nursing homes under Medicaid and Medicare, and requiring greater reporting of compensation of direct care and support staff, among other provisions. This Medicaid-related policy change was assumed in the federal Senate’s budget resolution.
- Rescinding or repealing the two-part CMS rule finalized in September 2023 and March 2024 that automates data verification and eliminates excessive paperwork, making it easier for families to apply and maintain coverage.
- Rescinding or repealing another rule finalized in May 2024 related to increased transparency and oversight for State Directed Payments, In Lieu of Services, and Medical Loss Ratios for MCOs.
Conclusion
As federal Medicaid policy debates continue, Kansas must prepare for potential shifts that could impact thousands of residents. The budget reconciliation process could bring sweeping changes to Medicaid, affecting funding, eligibility and expansion. If some or all of the policy changes were to be enacted, state policymakers would need to explore alternative funding mechanisms or state policies to address potential funding shortfalls to maintain health care access. Understanding these proposed changes and their consequences is vital for policymakers, health care providers and beneficiaries alike.
Stay tuned for updates and continued analysis from KHI as the budget reconciliation process continues.
Funding for Hill to the Heartland is provided in part by the Sunflower Foundation: Health Care for Kansans, a Topeka-based philanthropic organization with the mission to serve as a catalyst for improving the health of Kansans. KHI retains editorial independence in the production of its content and its findings. Any views expressed by the authors do not necessarily reflect the views of the Sunflower Foundation.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.