In Kansas, in the past two and a half years of the pandemic, several efforts have been made across the state to fund and better understand how to address vaccine equity and vaccine hesitancy. Below are only a few examples of those efforts.
- In November 2020, the Kansas Leadership Center (KLC) launched “Kansas Beats the Virus” in partnership with the State of Kansas, which was an effort to mobilize Kansas to generate local solutions that can lead to behavior-changing action. In 2020, the effort led to 851 meetings and the development of 827 action plans. In 2021, KLC partnered in a second phase with the Kansas Department of Health and Environment (KDHE) to provide tools and facilitators for communities to create local strategies to increase testing and vaccination rates resulting in 1,010 unique action projects that reached an estimated 1.35 million Kansans across the state. One of the outcomes was “most of the action projects were created by and directed toward racial and ethnic minority populations in Kansas.”
- In January 2021, two medical professionals, with community partners, in Garden City, created videos in several languages – English, Arabic, Tigrinya, Karen, Vietnamese, Rohingya, Quiche, Pleutdeutsch, Burmese, Spanish, and Somali – to address common concerns and questions around the COVID-19 vaccines.
- On March 10, 2021, Governor Kelly announced Dr. Ximena Garcia as her special advisor on COVID-19 vaccination equity. Dr. Garcia led the COVID-19 Vaccine Equity Taskforce.
- In May 2021, several counties – including Wyandotte and Shawnee – began going door-to-door in neighborhoods with high concentrations of Hispanic, Any Race, and Black populations to sign residents up for vaccines.
- In June 2021, the CDC awarded $31.9 million, including $11.6 million dedicated to rural efforts, to KDHE to address health and COVID-19 vaccine equity among populations at high-risk and underserved, including racial and ethnic minority populations and rural communities.
- In September 2021, KDHE commissioned NORC at the University of Chicago and the JUNTOS Center for Advancing Latino Health at the University of Kansas Medical Center Research Institute to conduct public opinion research on the sentiments of unvaccinated Kansans related to COVID-19 vaccines and testing. The findings were published in November 2021.
- On September 27, 2021, Governor Kelly announced a new grant program to “Increase the Reach,” which aimed to reach socially vulnerable populations and those experiencing low vaccination rates, including both racial and ethnic minority populations as well as rural communities.
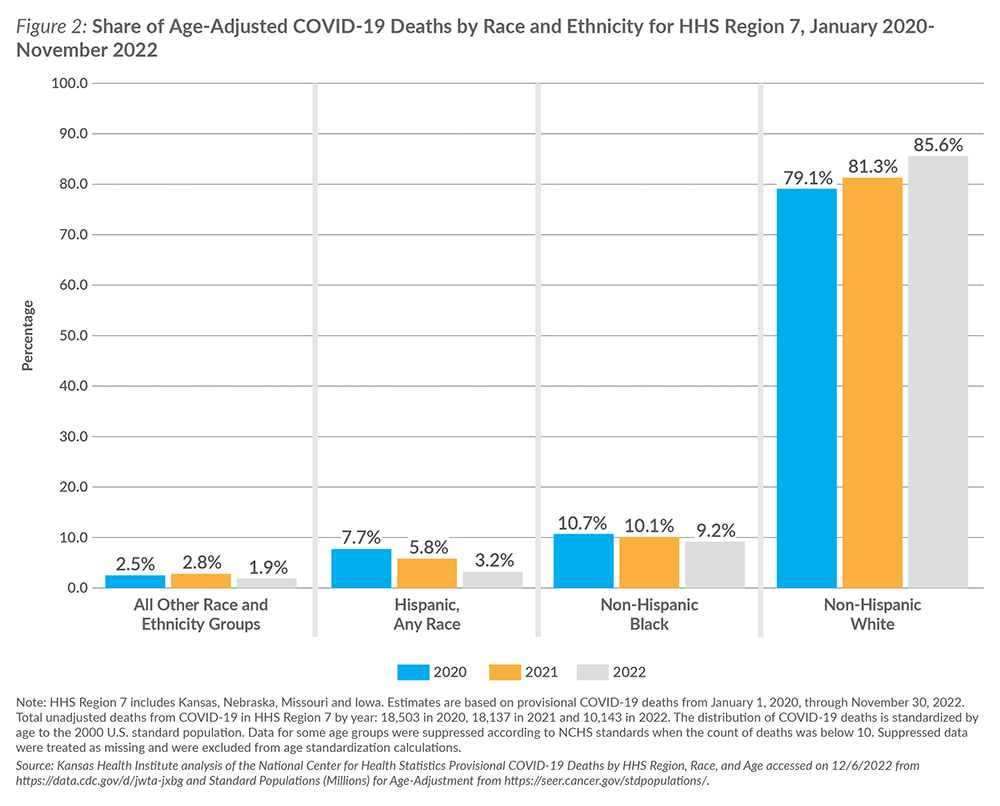
A few factors may contribute to the increase in the proportion of age-adjusted COVID-19 deaths among the non-Hispanic White population group. For instance, vaccination rates among non-Hispanic White individuals may have stagnated in the third year of the pandemic. In Kansas, KDHE data on COVID-19 vaccination demographics also show the gap has narrowed when compared to Black Kansans or eliminated when compared to Hispanic Kansans. There also are lower vaccination rates in some parts of the state. Another factor could be political ideology and its impact on vaccine uptake.
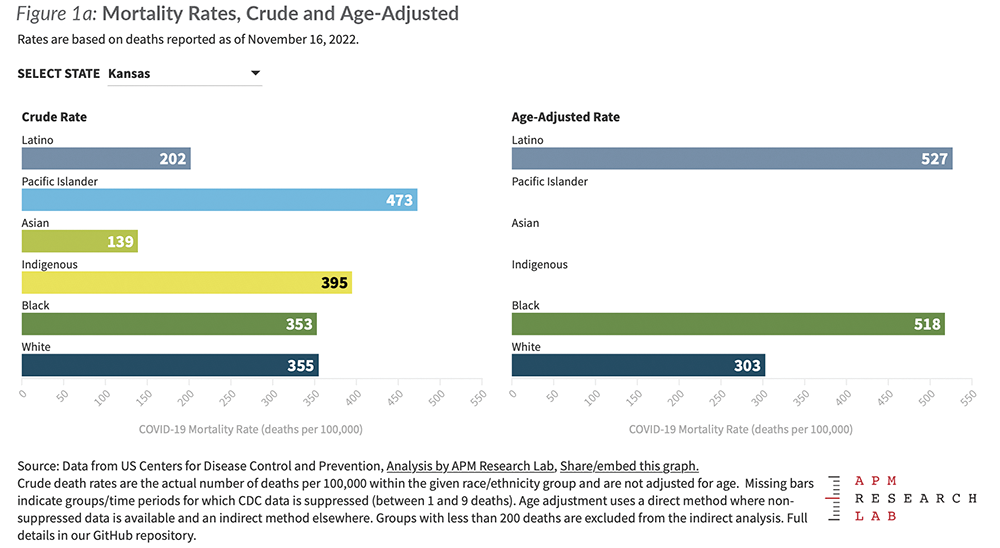
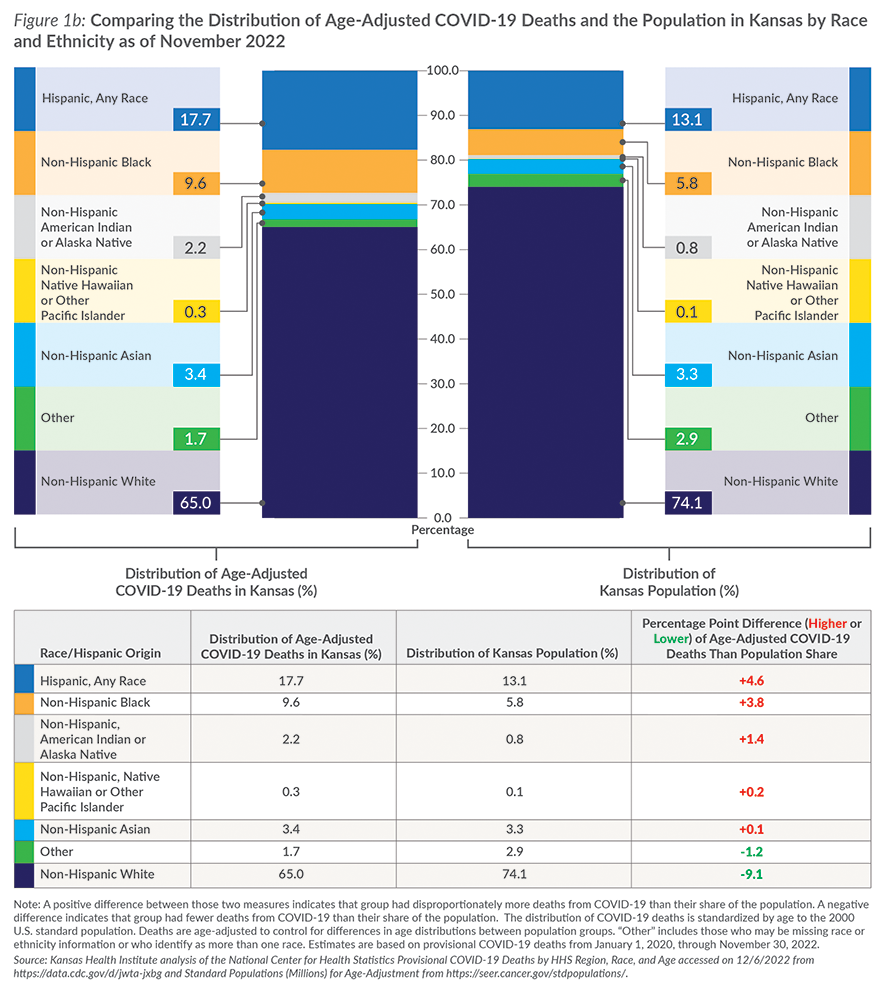
The bottom line: Data from the CDC show a higher burden of age-adjusted COVID-19 deaths among minority racial and ethnic groups in Kansas. Regionally – in Kansas, Missouri, Nebraska and Iowa – the trend is changing and overall deaths from COVID-19 have dropped in 2022. The share of age-adjusted deaths also has decreased for Hispanic, Any Race, individuals during the three-year period from 2020 to 2022. With a focus on health equity, understanding such trends and evidence-based efforts to identify successes, challenges and lessons learned could shape future actions.
Check back for more information as we continue to monitor the ongoing impact of COVID-19.