

What Happened to Health in Kansas?
Themes and Priorities Emerging from a Panel of Leaders and Experts in the Health of Kansas

“It was no surprise that Kansas was failing.”
That’s how one participant summed it up in our recent statewide study. And while the words are stark, they weren’t said out of cynicism. They came from a place of concern and commitment to improve.
Kansas used to rank among the healthiest states in the country. In 1991, we were eighth in America’s Health Rankings. Today, we’ve fallen into the bottom half. Our all-cause mortality rate, once better than the national rate, is now worse by more than 63 deaths per 100,000 people. We set out to understand why Kansas hasn’t kept pace with the rest of the country in the health rankings. What are the real, underlying drivers of our decline, and more importantly, what would it take to turn things around?
To answer these questions, we engaged 100 experts and leaders in Kansas’ health – public health officials, clinicians, researchers, community advocates, state and local government staff and others – in what is known as a Delphi study. A Delphi study is a structured method for building consensus among experts, using iterative rounds of surveys to distill collective judgment. Over three structured rounds, they shared their insights, debated what mattered most and ultimately prioritized the factors they believe are most important for reversing our state’s health ranking decline.
What we heard was clear: Kansas is facing deep, systemic health challenges, not just a series of isolated problems. But those systems can be reshaped. And Kansans are already showing what’s possible.
The Top Priorities: What Experts Said Is Driving Kansas’ Health Decline
Over the course of the Delphi process, participants identified 52 distinct issues contributing to Kansas’ health challenges. But four rose to the very top, including:
- Rural hospital and health care service closures
- Lack of Medicaid expansion
- Limited availability of mental health services
- Low public health funding
These were the issues that participants overwhelmingly supported across every metric. They were viewed as important, a priority for investing our collective effort and resources, and recognized by a majority of participants. What do they have in common? They’re not individual behaviors. They’re not narrowly focused programs. They focus on our core health policies and infrastructure – things that help shape health across a state.
We’re seeing the consequences. Kansas has the highest rate of rural hospitals operating at a financial loss than any other state. Without Medicaid expansion or interventions to increase private insurance reimbursement, many hospitals, especially in rural areas, are hanging on by a thread. And when hospitals close, communities suffer: fewer jobs, longer commutes for care, less economic opportunity and ultimately worse health outcomes.
Mental health was another urgent concern. Despite recent improvements, Kansas has ranked among the bottom states in access to care and mental health workforce capacity, and suicide rates have risen across Kansas, especially in rural and frontier communities.
“The high rates of suicides… in [rural counties] illustrate the severity of the mental health crisis in Kansas.”
Meanwhile, participants told us chronic underinvestment in public health in Kansas, one of the lowest per capita rates in the country, has left local systems fragmented and vulnerable. Participants described the public health system as “under attack,” “politicized” and struggling to regain public trust after COVID-19.
Going Deeper: The Flow of Health
To make sense of what we heard, we used a model called the Flow of Health. It’s a simple way of thinking about how health is shaped across three levels:
- Upstream: Policies, governance and cultural values
- Midstream: Individual socio-economic position and community conditions
- Downstream: The health care and public health systems
Participants emphasized that problems don’t sit in just one level. The issues at each level reinforce each other and when upstream problems go unaddressed, they ripple downstream, creating even bigger consequences.
We heard this pattern repeatedly across the study. Participants said what’s happening upstream in Kansas is setting the current for everything that follows, and the turbulence is showing up in our communities, our systems and our outcomes.
At the upstream level, participants described a state where policy choices often undermine health rather than support it. Medicaid expansion was the most prominent example. Participants said its absence has left Kansans with low income without coverage and weakened the financial foundation of rural hospitals. Others pointed to the chronic underfunding of public health, which has left many agencies under-resourced and unable to invest in long-term prevention. And beyond health-specific policies, participants flagged disinvestment in education and social programs as upstream forces that limit opportunity and drive inequities.
But the barriers aren’t just technical, they’re cultural and political. Participants described a governance landscape where health-promoting policies are blocked because they conflict with ideological beliefs.
Others noted that Kansas’ strong culture of individual responsibility, while admirable in many ways, can limit empathy and stall collective action. “There’s a whole ideology built around the idea that people’s circumstances are the direct result of their behavior,” one participant said, “and their fundamental goodness or badness.” That mindset, they argued, makes it harder to address systemic causes of poor health, or to support policies that help people meet basic needs.
At the midstream level, those structural and cultural forces show up as unequal opportunities for health. Participants described a landscape marked by poverty, racial and ethnic disparities, and geographic isolation, particularly in rural areas. These factors limit access to care, transportation, healthy food and economic opportunity. Yet participants also shared examples of hope: some communities are thriving, led by collaborative leaders who value all members of the community. Programs like Engaged Kansas and transportation initiatives in north central Kansas were offered as examples of strong leadership and innovative spirit.
Finally, at the downstream level, Kansas’ health systems are feeling the strain. Rural hospitals have closed (eight since 2015). Access to mental health services remains a challenge for many. Public health departments, especially smaller ones, struggle to meet performance standards due to low funding combined with a decentralized approach that leads to insufficient economies of scale.
Participants stressed the need for stronger leadership, more coordination and long-term investment. “We lack the [collective] leadership needed to frame up a coherent path forward,” one participant said bluntly.
In short, what’s happening in Kansas isn’t random. It’s the result of how systems interact, how policies, culture, funding and leadership shape the conditions where health either flourishes or falters. The good news? If systems can produce these outcomes, they can also be changed to produce better ones. The Flow of Health contextualized to Kansas’ experience is shown in Figure 1.
Figure 1. The Flow of Health Contextualized to Kansas’ Experience
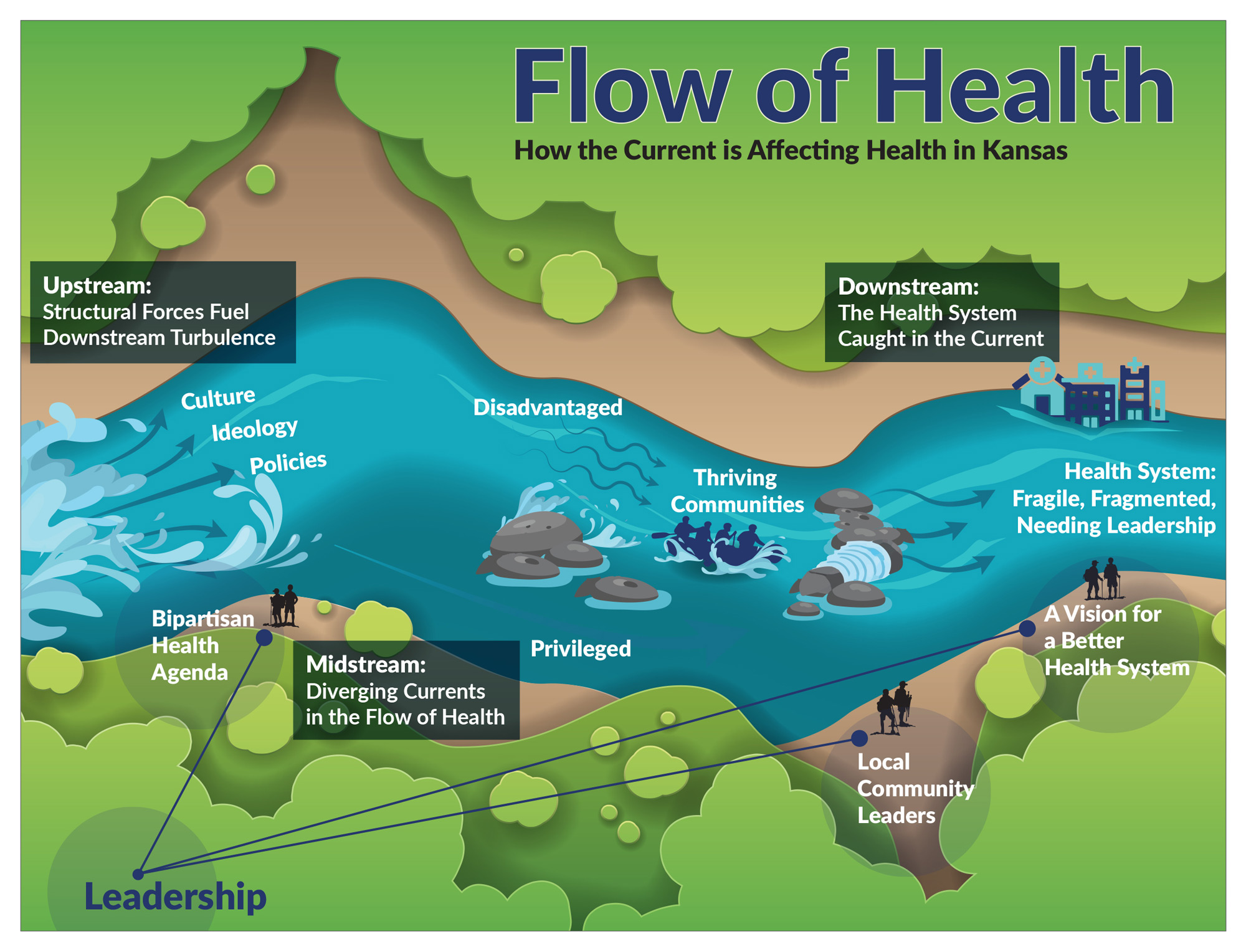
Note: The Flow of Health Contextualized to Kansas’ Experience was developed by the Kansas Health Institute by mapping themes identified through qualitative data analysis from the study onto the Flow of Health conceptual framework developed by the Kansas Health Institute based on a synthesis of socio-ecological frameworks developed by the World Health Organization, Bronfenbrenner, and Castrucci and Auerbach.
What Will It Take to Turn the Tide?
There doesn’t seem to be a silver bullet — one policy or program that accounts for the majority of Kansas’ health rankings decline. The results of the Delphi study show that Kansas’ health challenges are rooted in systems-level structures and repeated patterns. So where do the results tell us we should start? As Kansans, we start by recognizing that the status quo is not working and change is needed. Bringing people together across the political spectrum and across sectors, creating a shared vision for a positive future and building leadership in people beyond those with authority or titles can cultivate a culture that values everyone’s health and the systems and investments that produce population health in Kansas.
The Delphi study gave us more than a list of priorities. It gave us insight into the systems shaping Kansas’ health and what we can do next. We invite public health leaders, policymakers and partners across Kansas to use these findings to build a Kansas where health isn’t just a vision, but a shared reality. These reports, which I authored with Emma Uridge, Viktoria Sterkhova and Wen-Chieh Lin, reflect the collective insights of Kansas health experts and leaders and are meant to spark dialogue and action.
If you or someone you know needs support now, call or text 988 or chat 988lifeline.org.

About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.