Introduction
The 2017 legislative session will mark the first year of a two-year cycle. While issues from previous sessions—such as the status of the state’s psychiatric hospitals, Medicaid expansion and medical marijuana—will likely resurface, all will be in the form of new bills. Dozens of new faces in the Capitol also mean the Legislature itself will have a new character.
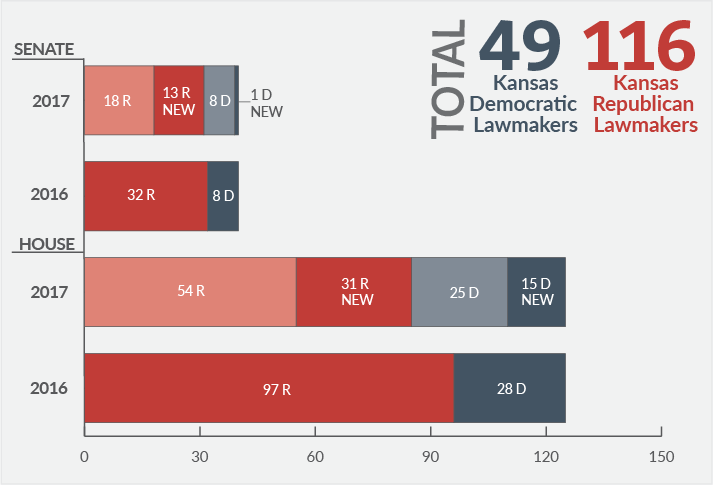
As a result of the general election in November 2016, the Kansas Senate has gone from 32 Republicans and eight Democrats to 31 Republicans and nine Democrats. Fourteen of the senators are new, although five of them were in the Kansas House in 2016. The Kansas House went from 97 Republicans and 28 Democrats to 85 Republicans and 40 Democrats. Forty-six of the representatives are new for 2017, but six of them have previously served in the House. (These numbers include the recent announcement of Rep. Marvin Kleeb’s retirement on Jan. 10 and the election of his successor, Abraham Rafie.)
KanCare
During the 2017 session, legislators will have the opportunity to debate and respond to a number of issues related to the current and future operation of the Kansas Medicaid program, known as KanCare.
KanCare 2.0
Although the initial three-year term of state contracts for the three KanCare managed care organizations (MCOs) ended December 31, 2015, the MCOs have continued to operate under an optional two-year extension of the original term of their contracts.
It was anticipated that the Kansas Department of Health and Environment (KDHE) would issue a new request for proposals (RFP) before the end of 2016 to select the MCOs that would be operating KanCare beginning on January 1, 2018. However, on November 18, 2016—during a meeting of the Robert G. (Bob) Bethell Joint Committee on Home and Community Based Services and the KanCare Oversight Committee—KDHE officials announced that the renewal process for KanCare was being placed on hold and the RFP was “delayed indefinitely.” On December 16, 2016, Lt. Governor Jeff Colyer announced that the state had renewed the existing MCO contracts and would not request new bids until late 2017. Colyer also stated these changes were the result of uncertainty regarding what the election of Donald Trump as president and Republican control of Congress might mean for state Medicaid programs.