Suicide Prevention
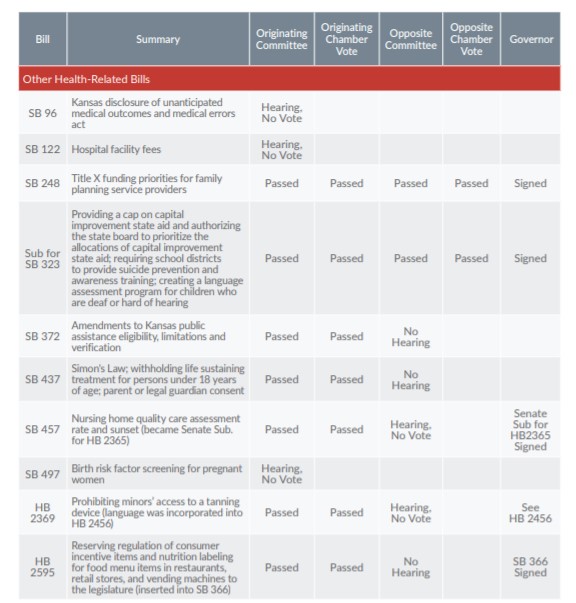
House Substitute for SB 323, introduced during the first week of the session and referred to the Senate Education Committee, required school districts to provide suicide awareness and prevention programming. Districts would be required to train school staff and develop a crisis intervention plan that would be implemented if staff identify students considering suicide. Gov. Brownback signed the bill on May 11.
Immunity for Minors Seeking Medical Assistance
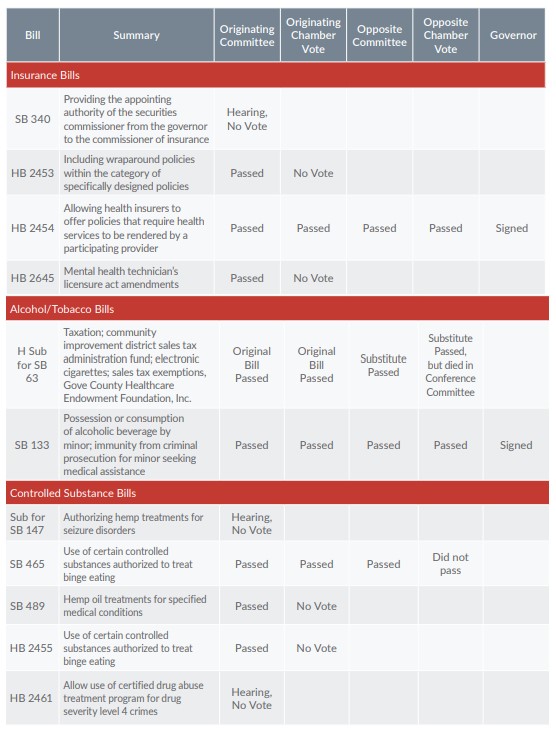
Early in the session, the governor signed SB 133, which provides immunity to minors regarding the possession or consumption of alcoholic beverages if they contact law enforcement or emergency medical services to request assistance for themselves or another person. The new law is intended to protect minors from prosecution if they report alcohol poisoning. Proponents hope it will prevent deaths of underage drinkers. Opponents of the bill would like to amend the law in 2017 to add a parental notification requirement and provisions for repeat offenders.
“Narrow Network” Insurance
Under HB 2454, health insurers in Kansas may now offer policies that require enrollees to obtain health services only from participating providers, with the exception of emergency services. The use of so-called “narrow networks” is one of the features that insurers use to control health care costs. The bill was introduced during the first week of the session and signed by the governor in March.
Tax on Electronic Cigarettes
House Substitute for SB 63 would have delayed the effective date of a new tax enacted in 2015 on the privilege of selling or deal in in electronic cigarettes from July 1, 2016 to January 1, 2017. The bill passed both chambers but died when the conference committee report was not adopted, so the tax began on July 1.
Simon’s Law
Simon’s Law (SB 437) was introduced to forbid health care facilities or providers from withholding life-sustaining procedures, food or medication from any patient under age 18 without written permission from a parent or legal guardian. The bill also prohibited physicians from instituting a do-not-resuscitate (DNR) order on a minor without permission from a parent or legal guardian. The bill was named after the minor son of Missouri native Sheryl Crosier, whose son died due to a DNR that she and her husband did not know about. The bill passed the Senate, but did not advance out of the House Committee on Federal and State Affairs.
Food Item Labeling
One of the more contentious hearings of the 2016 session was on HB 2595, which related to local jurisdictions’ authority on food labeling and regulation of food items. Proponents want the Legislature to make food labeling standards statewide instead of allowing cities, counties and school districts to create local standards. Opponents discussed the definition of “political subdivision,” which they believed would also include groups such as schools and food policy councils, and expressed concerns that the bill would prevent local efforts to create healthy food environments, promote healthy eating and increase access to healthy foods, especially for children. Language from HB 2595 was inserted into SB 366, which was signed into law on May 17, 2016.
Disclosure of Medical Errors
SB 96, introduced in the Senate Judiciary Committee, would have required health care providers to disclose events resulting in unanticipated outcomes or medical errors to patients and their families or representatives. Opponents of the bill, including the Kansas Medical Society, expressed concerns that, without protection for malpractice liability for providers, the bill could encourage the filing of lawsuits. The bill died in committee.
Budget
The 2016 Legislature was dominated by discussion of how the budget would be affected by revenues that came in below original forecasts, as well as the Kansas Supreme Court’s ruling that required a special session to address K-12 education funding. By the end of the original session, the Legislature had adopted a revised budget that required the governor to make nearly $100 million in additional reductions in FY 2017 in the form of allotments.
Notable reductions in the allotments included:
Reimbursement reductions around 4 percent for many Medicaid providers ($38.2 million)
Exempt from this cut were 95 critical access and other rural hospitals, as well as providers of home and community-based services for elderly and people with disabilities.
-
- Other KanCare spending cuts ($18.2 million) Included a half-percent reduction—from 1.0 percent to 0.5 percent—in the managed care profit margin built into KanCare rates.
- Higher education cuts ($30.7 million) Included cuts of $7.0 million to the University of Kansas, $3.7 million to the University of Kansas Medical Center, and $5.2 million to Kansas State University.
- Reductions averaging 8 percent for Children’s Cabinet programs ($3.4 million)
Other changes had already been adopted by the Legislature based on recommendations in the governor’s budget, including ending the health homes project for KanCare members with serious mental illnesses (estimated to save $13.4 million) and removing the statutory prohibition on step therapy in the Medicaid program (estimated to save $10.6 million).
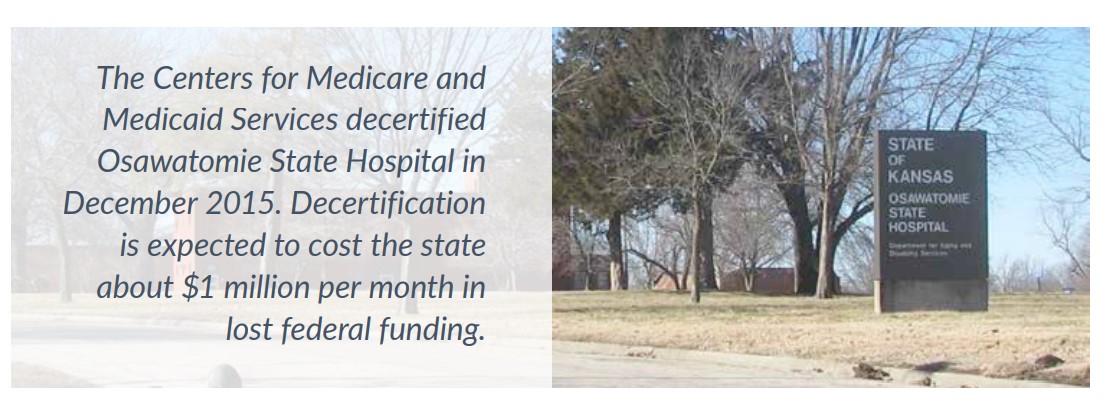
The budget bill included some provisions to raise spending in health-related areas, most notably an increase in allocations for the state psychiatric hospitals in Osawatomie and Larned, and an increase in funding for Department of Children and Families (DCF) to recruit and retain social workers.
The Legislature also approved the sale of the Kansas Bioscience Authority (KBA) assets, estimated to bring in $25 million. The KBA was founded in 2004 to invest in bioscience startup companies.