Introduction
During the 2015 session, Kansas legislators introduced and debated a number of issues related to health policy. Also in 2015, the Kansas Health Institute (KHI) for the first time published a brief summarizing the health policy issues considered during the session. This new brief continues that work by previewing health-related issues that may arise during the upcoming 2016 session.
Health policy advocates and health care providers are likely to once again ask legislators to consider Medicaid expansion. Legislators also will be assessing the operation and ongoing implementation of KanCare, the Medicaid managed care program in Kansas.
The Kansas Legislature operates on a two-year cycle; bills and resolutions introduced during the first year of the cycle (odd-numbered years) remain on the docket during the second year, which is also an election year. Consequently, bills and resolutions introduced but not passed during the 2015 session are still in play for the 2016 session. Health-related bills debated during 2015—including cannabis (marijuana) oil, liquor sales in grocery and convenience stores, and scope of authority and practice for a number of health care professionals—may again be considered in 2016. This brief also introduces some new topics that legislators may consider.
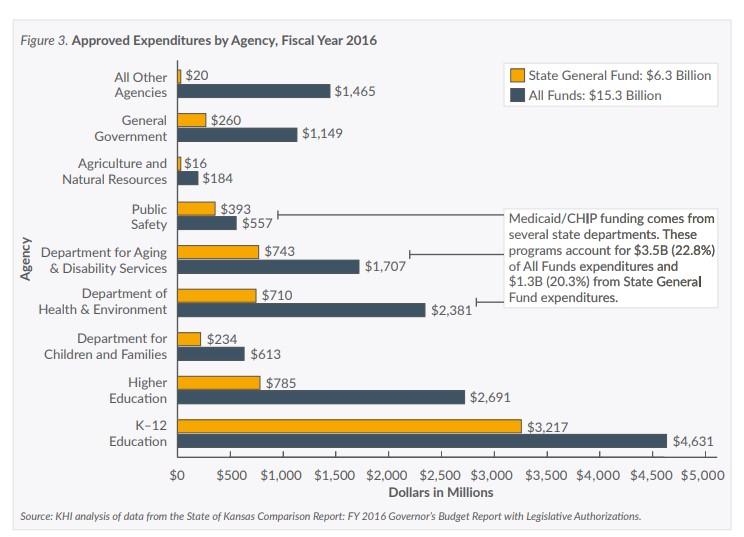
A presentation of the approved state budget and health-related spending for fiscal year 2016 is included here, because budget issues will likely occupy much of the legislature’s time and attention as adjustments are made to accommodate for lower than expected revenue collections. These debates may have a direct impact on the number and type of health policy issues legislators choose to address in 2016.
KanCare
Recent analysis shows that KanCare enrollment rose by 6.0 percent between 2013 and 2014, even though Kansas did not expand Medicaid as allowed under the Affordable Care Act (ACA). The initial three-year term of state contracts for KanCare managed care organizations (MCOs) ended December 31, 2015. Now, the state has the option to renew the contracts for up to two one-year periods. Therefore, legislators will likely be seeking more information and data regarding the outcomes and success of KanCare as they continue to review the program and make changes necessary for the future.
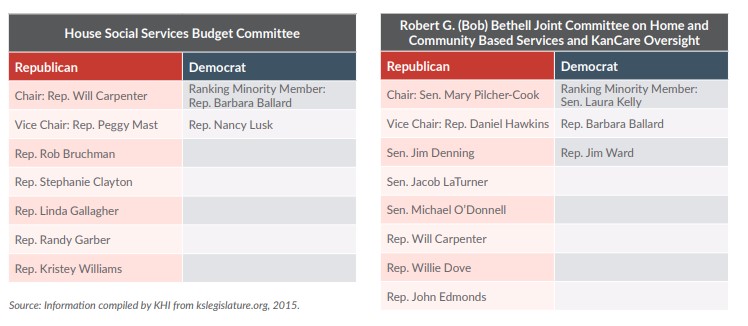
Under Senate Substitute for HB 2042, which passed in 2015, the Senate president will appoint two new members to the KanCare oversight committee, which is officially named the Robert G. (Bob) Bethell Joint Committee on Home and Community Based Services and KanCare Oversight. At least one of the new members must come from the Senate Ways and Means Committee. Under the same bill, the Speaker of the House will appoint a member to the oversight committee that must come from the House Appropriations Committee.
Under Senate Substitute for HB 2149, which also passed in 2015, the Medicaid Drug Utilization Review Board will enact guidelines on medications used to treat mental illness, including prior authorization. The Kansas Department of Health and Environment (KDHE) has stated that prior authorization requirements will likely save $8 million in fiscal year 2016. The law also established the Mental Health Medication Advisory Committee, which is charged with developing and recommending guidelines to the Review Board. Mental health advocates have expressed concerns that the requirements will increase administrative costs and delay medications for patients. Those advocates will have the opportunity to respond when prior authorization guidelines are submitted to the Review Board for consideration. The Advisory Committee has met twice since the end of the 2015 session and its recommendations may be considered at the Review Board’s next meeting in January 2016. Depending on the number and type of prior authorization guidelines recommended by the Advisory Committee, mental health advocates may ask legislators to review the guidelines or reconsider the Review Board’s authority to enact those requirements without legislative action.
Medicaid Expansion
As many as 150,000 additional Kansans might be immediately eligible for coverage if the state expands Medicaid up to 138 percent of the federal poverty level, as allowed by the ACA.
Since the end of the 2015 session, a number of events have raised the profile of the Medicaid expansion debate. The Kansas Hospital Association, for example, has signaled its intent to introduce a detailed plan for expansion and has released the results of a study showing that additional federal Medicaid dollars flowing into the state would boost the Kansas economy. The closing of Mercy Hospital in Southeast Kansas—which has been attributed, in part, to not expanding Medicaid—has raised concerns about the possibility of additional rural hospital closings. A KanCare forum held in Wichita recently provided an opportunity for legislators and health care advocates to hear representatives from Indiana speak about the alternative expansion plan implemented by their Republican governor and legislature.
Recent polls show that a majority of Kansans support some form of expansion. The Wichita Metro Chamber of Commerce—citing costs incurred by the business community to cover the losses experienced by hospitals providing care to uninsured adults—voted to add expansion to its list of priorities for 2016.