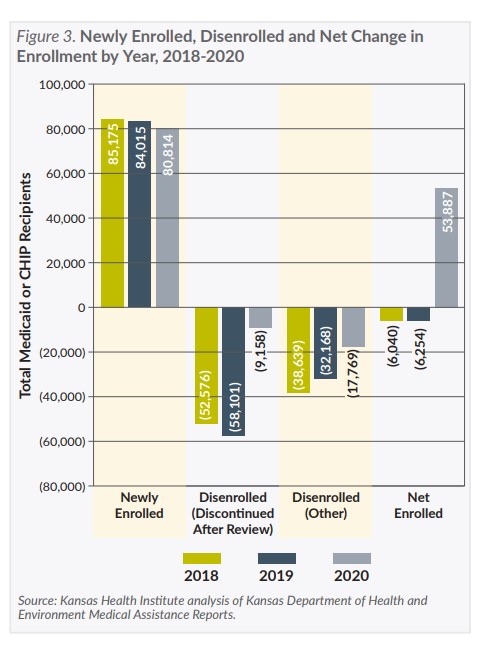
While the number of new enrollees is lower since the pandemic began, the total change in enrollment, which had been decreasing, increased sharply in 2020. Since the number of new enrollees has not increased, this implies that fewer people are disenrolling and the increase in KanCare enrollment during the COVID-19 pandemic has been driven primarily by the policy decision to delay acting on annual reviews until after the COVID-19 public health emergency ends.
Discussion
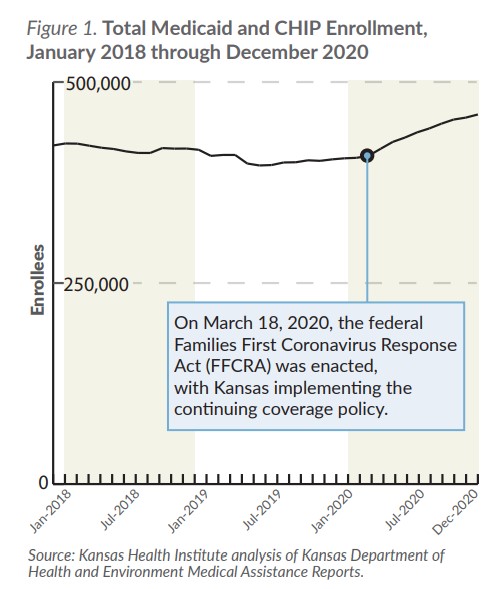
The continuing coverage policy has many short-term benefits. In addition to covering the cost of COVID-19 vaccines and treatment for KanCare members, the policy has extended eligibility for many enrollees who would have otherwise been disenrolled, possibly without another health insurance option in the midst of a pandemic.
The continuing coverage policy also has reduced the state’s overall KanCare costs. Because the state contracts with managed care companies to provide KanCare benefits, the cost for additional enrollees is largely fixed. The 6.20 percentage point increase in federal funds for the entire KanCare population has more than offset costs for the additional enrollees and for COVID-19 testing and treatment for KanCare members.
Volume 1 of the FY 2022 Governor’s Budget Report states that the increased FMAP, which was retroactive to January 1, 2020, had decreased the required state share of Medicaid expenditures by approximately $153.2 million in FY 2020 and would reduce expenditures by an estimated $161.4 million in FY 2021, assuming the increased FMAP expired on March 31, 2021. However, the Biden Administration extended the COVID-19 public health emergency another 90 days and has announced intentions to continue extending it through at least the end of 2021, so it is expected that the increased FMAP also will continue until then.
The long-term effects of the increase in enrollment on the KanCare program and state budget are less certain. Once the public health emergency ends, annual reviews will resume for tens of thousands of KanCare enrollees while the additional federal financial support for maintaining their enrollment ends. Many of the enrollees who have retained eligibility will be disenrolled. Some will re-enroll and others will be covered through other insurance or become uninsured. If the economic effects of the pandemic outlast the health crisis, a rapid return to pre-pandemic KanCare enrollment may be unlikely.