

Make America Healthy Again
A Deeper Look Into the Trump Administration’s National Health Initiative

Introduction to Make America Healthy Again (MAHA)
The term “Make America Healthy Again” (MAHA) gained prominence during the 2024 presidential campaign cycle. It initially emerged from health-focused messaging promoted by Robert F. Kennedy Jr. during his independent presidential campaign. Following Kennedy’s suspension of his campaign and his subsequent endorsement of then former President Donald Trump in August 2024, the phrase began to gain broader public attention.
After his reelection, President Trump announced Kennedy as his nominee for United States Health and Human Services (HHS) secretary. Kennedy was confirmed to the role on Feb. 13, 2025, following a 52-48 vote, and was sworn in the same day. Also on Feb. 13, the White House issued Executive Order (EO) 14212: Establishing the President’s Make America Healthy Again Commission, which formally created the MAHA Commission, outlining its purpose, responsibilities and deliverables. Since his confirmation, Kennedy has initiated reforms within HHS to align with the vision of MAHA.
The MAHA Commission: Background Context and How Kansas Compares
EO 14212 frames chronic disease and related conditions as urgent national health, economic and security challenges. It highlights the impact of nutrition, environmental exposures and lifestyle factors on health, particularly among children, and emphasizes that Americans are becoming sicker at younger ages. The order calls for a shift in the U.S. health care system from managing disease to promoting health across the lifespan and tasks the commission with reviewing health trends and providing recommendations to improve national health outcomes.
Purpose and Goal of the MAHA Commission
Purpose: To create the highest quality of life and build the safest, wealthiest, healthiest and most vital communities anywhere in the world by addressing the root causes of America’s escalating health crisis.
Goal: To lower chronic disease rates, especially in children, by shifting national focus toward prevention, healthy lifestyles and a health-promoting health care system, grounded in scientific integrity.
Health Measures
Lagging Life Expectancy
EO 14212 highlights that American life expectancy has lagged behind other high-income countries, noting that pre-COVID-19 life expectancy was 78.8 years compared to an average of 82.6 in peer nations. Recent Centers for Disease Control and Prevention (CDC) data show while U.S. life expectancy partially rebounded to 78.4 years in 2023, it remains below pre-pandemic levels and behind peer nations such as Canada, France, Japan and the United Kingdom, where on average life expectancy is near pre-pandemic levels at 82.5 years.
Kansas has largely mirrored these national trends. In 2019, life expectancy in Kansas was 78.2 years. By 2021, it saw a 2.2-year decline, as life expectancy nationwide also declined. More recent state-level data has not yet been published, making post-pandemic comparisons unclear.
Chronic Disease Prevalence
Chronic disease is a public health concern nationally and in Kansas. EO 14212 cites data from a 2017 RAND Corporation study which estimates that 6 in 10 Americans (60 percent) had at least one chronic condition and 4 in 10 (42 percent) had more than one chronic condition. A 2020 CDC report estimates approximately 51.8 percent (129 million) of civilian, noninstitutionalized adults in the U.S. have at least one chronic condition and 27.2 percent (68 million) have two or more.
Asthma is also a concern. EO 14212 states that in 2021, asthma was more than twice as common in the United States than in many European, Asian and African countries. This aligns with a January 2025 Lancet study using Global Burden of Disease 2021 data which found the United States had among the highest age-standardized asthma prevalence rates globally. Some contributors to asthma prevalence cited in the study included social and economic conditions affecting health outcomes, high body mass index (BMI) and smoking. According to the America’s Health Rankings (AHR) 2024 report, 9.9 percent of Kansas adults report ever being told they have asthma, slightly below the U.S. rate of 10.3 percent. Together, these statistics reflect the chronic disease landscape in Kansas and nationwide.
Cancer Incidence and Mortality
EO 14212 cited cancer statistics from a recent global study by researchers at Huazhong University of Science and Technology in Wuhan, China, which found the U.S. had the highest age-standardized incidence rate (ASIR) of cancer in 2021 among 204 countries and territories — 3,304.9 cases per 100,000 people. This rate was more than double Canada’s, which had the second highest ASIR. The study, published in BMC Journal of Hematology & Oncology, also found that cancer incidence in the U.S. increased by 88 percent from 1990 to 2021. However, this study has raised concerns among some cancer epidemiologists about the reliability and comparability of data. In contrast, the International Agency for Research on Cancer reported the United States had an ASIR of 367.0 cases per 100,000 people in 2022, the fourth highest rate globally following Australia, New Zealand and Denmark. Regardless of variations in data sources and methodology, cancer remains a major public health concern.
In Kansas, the all-cancers overall incidence rate was 454.2 per 100,000 people during 2017–2021, according to the Kansas Department of Health and Environment. These state-level data reflect broader concerns outlined by the MAHA Commission, which identifies cancer as a persistent and growing public health challenge.
Mental Illness Prevalence in Adults
EO 14212 also elevated mental health as a key priority. Within the executive order, the Trump Administration estimates that 1 in 5 adults living in the United States live with a mental illness. This is consistent with National Institute of Mental Health (NIMH) data, which states that in 2022, 59.3 million (23.1 percent) U.S. adults live with a mental illness. According to AHR, 15.4 percent of the U.S. population experience frequent mental distress, defined as 14 or more days of poor mental health each month. Kansas closely follows this experience, with 15.6 percent of Kansans reporting frequent mental distress. These figures underscore the widespread and persistent nature of mental health challenges, both nationally and in Kansas, reinforcing the need to address mental health alongside physical health conditions.
Child Health
EO 14212 highlights the growing health challenges facing children in the U.S., estimating that 30 million children (40.7 percent) live with at least one health condition. This aligns with CDC’s report stating that more than 40 percent of school-aged children and adolescents have at least one chronic condition. The executive order also raises concern over other conditions, noting that 18 percent of late adolescents and young adults are impacted by non-alcoholic fatty liver disease (NAFLD), aligning with a 2021 Johns Hopkins study, and stating that nearly 30 percent of adolescents are prediabetic, closely mirroring 2023 CDC data estimating 32.7 percent. According to EO 14212, around 40 percent of adolescents are overweight or obese, comparable to CDC data from 2021 that indicate a combined overweight and obesity rate of 35 percent, slightly trailing the statistic reported in EO 14212. The order also raises concerns about the rising use of medication for attention deficit hyperactivity disorder (ADHD), citing 3.4 million children receive medication; CDC 2022 data support this finding, with 7 million diagnoses and 53.6 percent (3.8 million) receiving medication. EO 14212 also reports that 1 in 36 are affected by autism spectrum disorders (ASD), which is consistent with data from an April 2025 CDC Morbidity and Mortality Weekly Report (MMWR).
Health System Performance
EO 14212 frames declining U.S. health outcomes as evidence of a failing health care system that prioritizes disease management over a more holistic vision of health and well-being. The order emphasizes that, despite spending $4.5 trillion in health care expenditures annually, these expenditures have not resulted in better outcomes at the system or individual level. The order calls for a national refocusing of health to lower chronic disease rates and ending childhood chronic illnesses to improve the health of Americans and strengthen the economy and security of the United States.
U.S. Health System Performance
Findings from the Commonwealth Fund’s recent report, Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System, reinforce this concern. In its comparison of health care system performance across ten high-income peer nations, including the United States (U.S.), Australia (AUS), Canada (CAN), France (FRA), Germany (GER), the Netherlands (NETH), New Zealand (NZ), Sweden (SWE), Switzerland (SWIZ) and the United Kingdom (UK), the U.S. ranked last overall (Figure 1). Conversely, health care spending was highest in the U.S., a pervasive issue since the 1980s. In 2022, health care spending as a percentage of gross domestic product (GDP) in the U.S. was 16.9 percent. The same statistic for all other countries in the report ranged from 9.8 percent to 11.9 percent. Despite the United States’ high health care spending, the U.S. continues to deliver worse health outcomes than its peers, a pattern reflected across nearly all domains analyzed in the Commonwealth Fund report.
Figure 1. Health Care System Performance, by Country, 2024
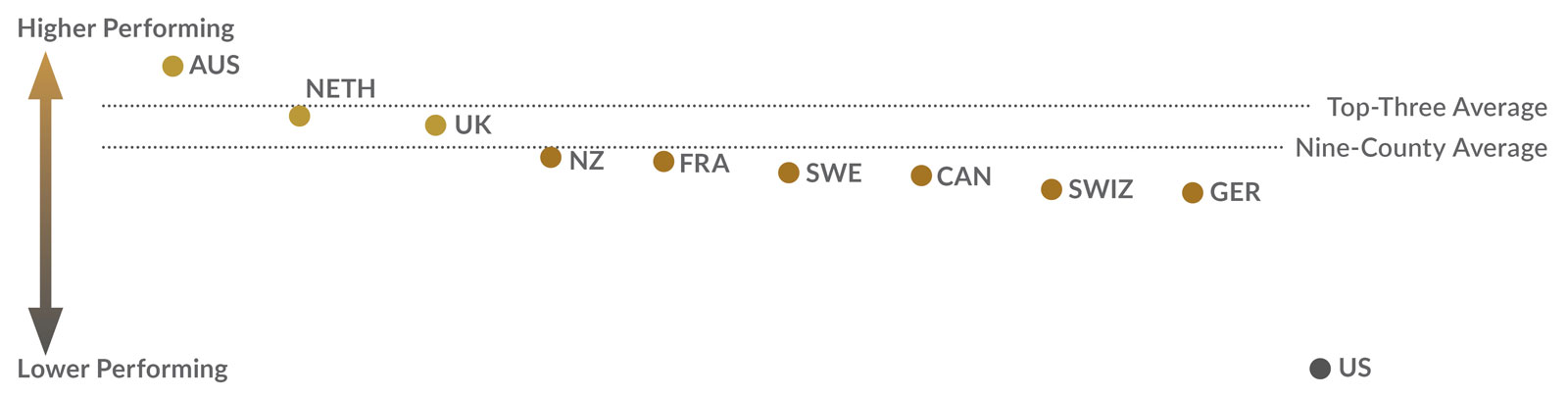
Source: Blumenthal, D., et al. (2024). Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System. Commonwealth Fund.
The report explored five key domains of health care system performance — access to care, administrative efficiency, care process, equity, and health outcomes (Figure 2). The U.S. ranked lowest overall, with lower rankings in access to care, equity, and health outcomes. It ranked second in care process, reflecting strengths in preventative services and patient safety. It highlights continued challenges in achieving equitable access, administrative efficiency and improved health outcomes despite high spending.
Figure 2. Ranking Five Key Domains of Health Care System Performance, by Country, 2024
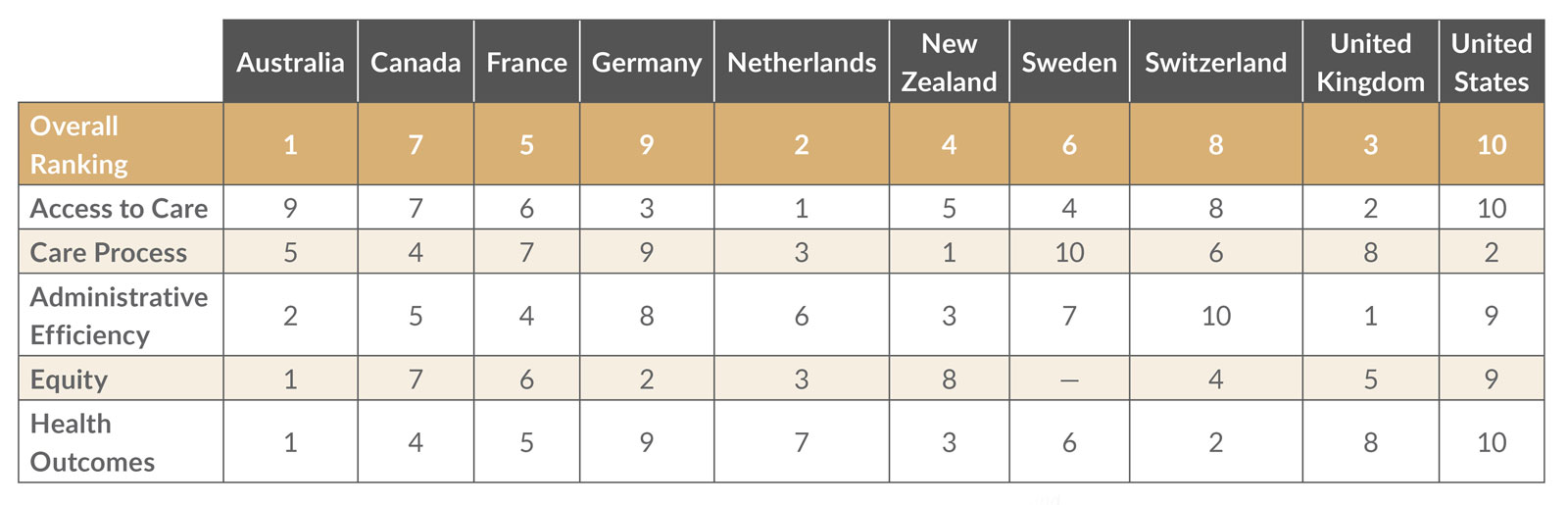
Source: Blumenthal, D., et al. (2024). Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System. Commonwealth Fund.
Kansas Health System Performance
While the Commonwealth Fund’s Mirror, Mirror 2024 report focuses on international comparisons, its findings highlight challenges that also exist within the United States. State-level performance varies widely, revealing that some states perform better or worse than the national average despite operating under the same broader national health care system. In Kansas, the Commonwealth Fund’s 2025 Scorecard on State Health System Performance ranked Kansas 33rd overall and sixth among the plains states (Figure 3). Kansas especially underperforms in Access and Affordability, Avoidable Hospital Use and Cost, and Income Disparity, driven in part by high rates of uninsurance among low-income adults and high out-of-pocket medical spending. Income disparity is calculated as the difference in performance on selected health indicators between low-income residents (below 200 percent of the federal poverty level (FPL)) and higher-income residents (above 400 percent of the FPL). However, Kansas performs better on some child-focused indicators in the Prevention and Treatment domain. These patterns echo the broader national challenges of inconsistent access, disparities, and uneven outcomes.
Figure 3. State Health System Performance, 2025
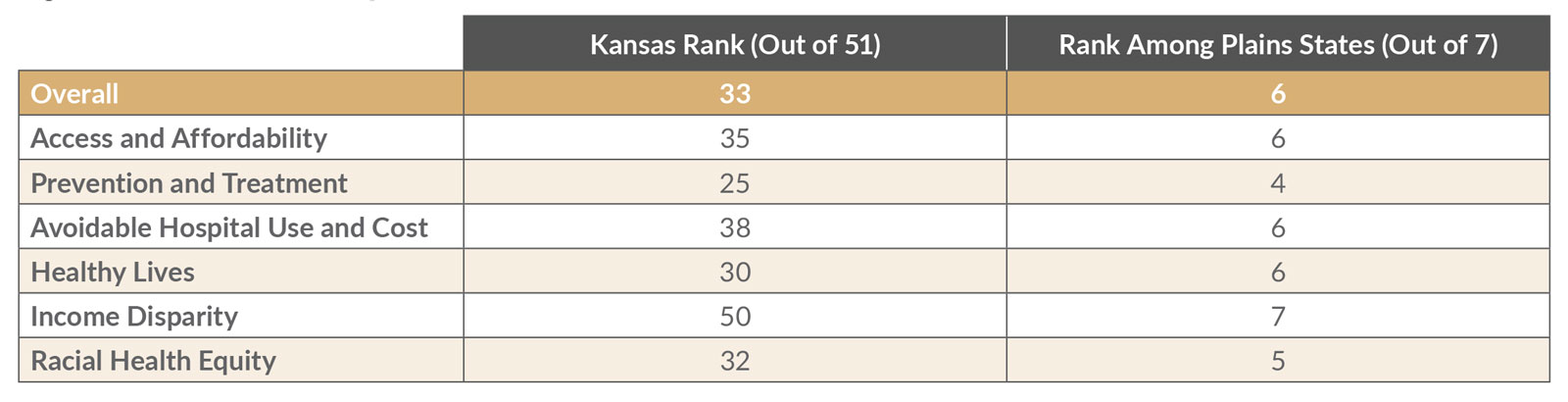
Note: To access state profiles, select “State Profiles (ZIP)” in the downloads section on the report’s main page. For this report, the Plains states are defined as Iowa, Kansas, Nebraska, Minnesota, Missouri, North Dakota, and South Dakota. Each domain is scored using multiple indicators that determine a state’s performance relative to others. Access and Affordability measures rates of insurance coverage, cost-related barriers to care, medical debt, and out-of-pocket burden. Prevention and Treatment measures use of preventive services, mental health care, and quality of care across settings. Avoidable Hospital Use and Cost measures preventable visits, readmissions, per-person spending, and the share of spending on primary care. Healthy Lives measures health outcomes such as premature death, infant mortality, and preventable conditions. Income Disparity is the difference in performance on selected indicators between the state’s lower-income and higher-income populations. Racial Health Equity is the difference in performance on selected indicators across racial and ethnic groups.
Source: Radley, D., Kolb, K., and Collins, S.R. (2025). 2025 Scorecard on State Health System Performance.
MAHA Commission Responsibilities
EO 14212 established the Make America Healthy Again Commission to lead federal efforts in addressing chronic disease, with a particular focus on children. The Commission is tasked with studying the causes and prevalence of chronic illness and mental health conditions, advising the President on effective public communication, and providing policy recommendations to improve national health. It is responsible for producing two major reports — the Make Our Children Healthy Again Assessment (MAHA Report), released on May 22, 2025, which identified poor diet, environmental exposures, physical inactivity, chronic stress and overmedicalization as key drivers of childhood chronic disease. The second report, the Make Our Children Healthy Again Strategy, is on track for submission to the White House by Aug. 12, 2025, with public release expected in the coming weeks.
Looking Ahead
The release of the Make Our Children Healthy Again Strategy will mark a key moment in the federal effort to address chronic disease. How these recommendations are implemented and whether they lead to changes that improve outcomes in states like Kansas will require continued observation. As new developments occur, further analysis will help clarify the MAHA Commission’s role in shaping future public health policy.
Access this publication in the Documents & Downloads section.
Stay tuned for further updates on policy shifts that may affect health programs and services in Kansas. For related work on how federal policies could impact Kansans, please check out Hill to the Heartland.
Funding for Hill to the Heartland is provided in part by the Sunflower Foundation: Health Care for Kansans, a Topeka-based philanthropic organization with the mission to serve as a catalyst for improving the health of Kansans. KHI retains editorial independence in the production of its content and its findings. Any views expressed by the authors do not necessarily reflect the views of the Sunflower Foundation.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.