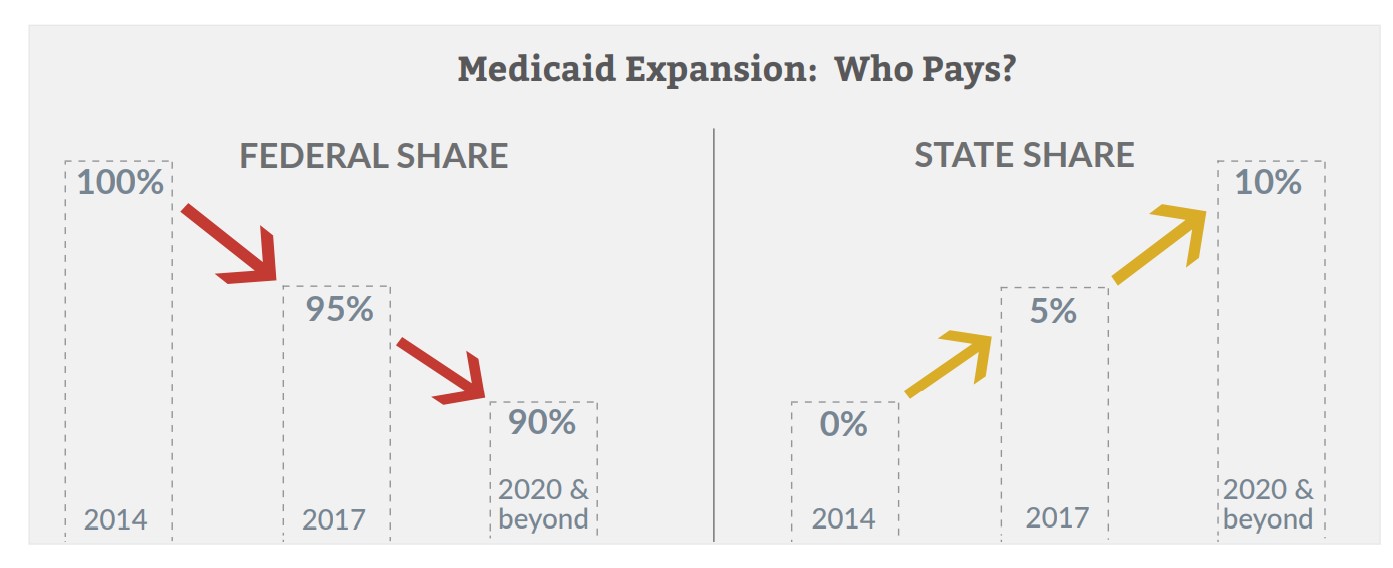
Federal costs. As an incentive to states that have not yet expanded, the Obama administration has proposed that the federal government pay 100 percent of the costs of newly eligible enrollees for the first three years of their expansion, regardless of when it begins. However, per-member costs for newly eligible adults in 2015were 49 percent higher than federal projections, raising questions about whether the next Congress or the new President would support such a proposal. How expansion affects health and quality-of-life. Though many states have expanded Medicaid, little data currently exist on the impact expansion has had on health outcomes. A widely cited, pre-ACA example of the health effects of Medicaid expansion is the Oregon Health Insurance Experiment. After randomly selecting and enrolling thousands of Oregonians from a waiting list to the state’s limited-availability Medicaid program in2008, researchers were able to evaluate the differences in health outcomes between the “selected enrollees” and the “non-enrollees” still on the waiting list after two years of the program.
The study found an overall increase in use of all types of health care services by the selected enrollees, including increased use of preventive care and prescription drugs, cholesterol monitoring and mammogram screenings, higher rates of diabetes detection and management, and reduced rates of depression. Although the selected enrollees showed increased use of health care services, there was no significant improvement in objective health measures such as blood pressure, cholesterol or blood sugar levels. However, the selected enrollees were more likely to report their health status as “good to-excellent” and were less likely to report financial hardship related to medical expenses as compared to the non-enrollees.
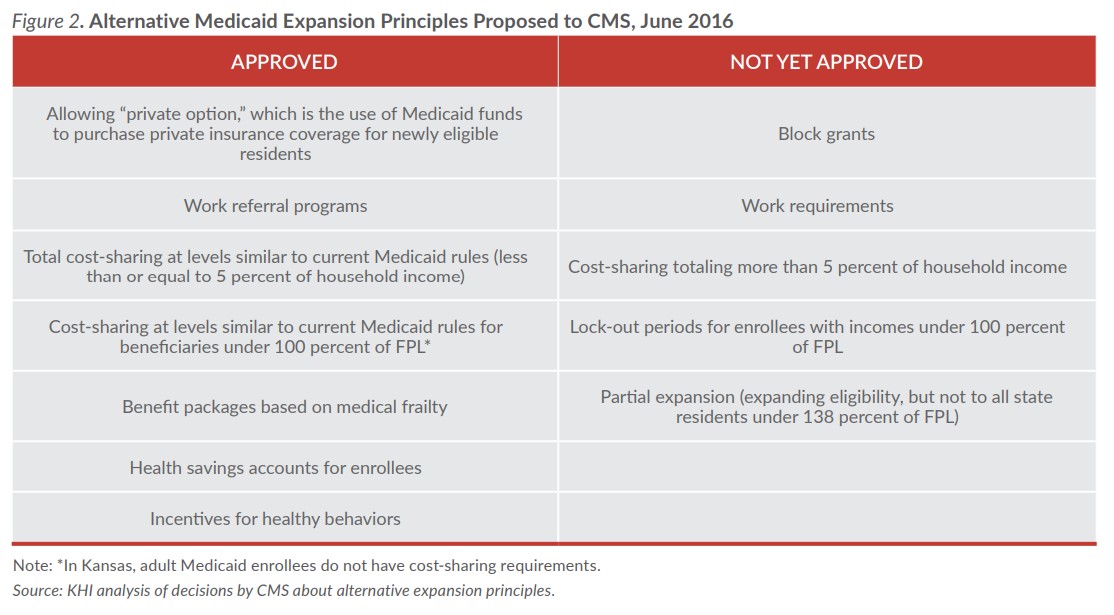
How the expansion population uses services. An often stated goal of Medicaid expansion is to decrease the number of emergency department (ED) visits, as many individuals who may have sought care through the ED would now have access to primary care physicians. The Oregon study also evaluated health care utilization and found that the selected enrollees had more office visits in the previous year than the non enrollees. However, they also found an increase in the number of ED visits, including non-emergency or primary care visits. This finding suggests that insurance coverage may not immediately impact the behaviors of the previously uninsured. What alternative programs might include. Thus far, states have been allowed to include a number of new principles in their alternative Medicaid expansion programs, including having enrollees with incomes below the federal poverty level pay premiums and/or copayments, creating health savings accounts, providing incentives for healthy behaviors, and using Medicaid funds to purchase private insurance. One of the most heated debates between states and CMS has been over work requirements, which the Obama administration has not allowed. The election of a new president in November may bring a new stance on this provision, which could lead some of the remaining non-expansion states to reconsider a state specific plan.
Conclusion
As states continue to weigh the pros and cons of Medicaid expansion, early experiences in other states can help inform legislative decisions. To date, expansion states have seen higher-than-expected Medicaid enrollment, but cost results have been mixed, and there is, so far, limited data on the effect of expansion on health outcomes.
As time passes and more results from early expansion states become available for analysis, policymakers who are still considering Medicaid expansion may find clearer information to inform their decisions.
Access additional State Spotlights in the Documents & Downloads section.