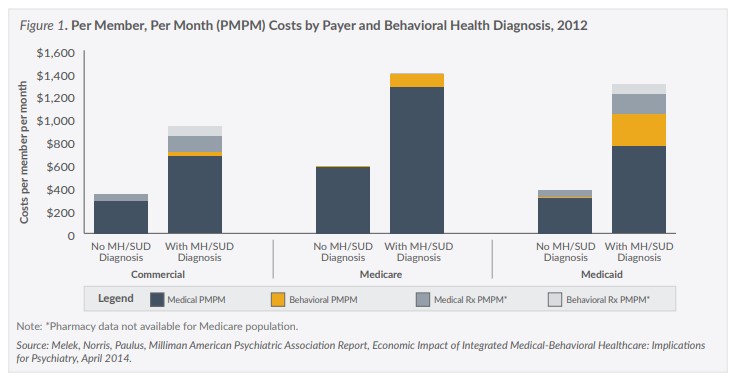
In 2013, the Sunflower Foundation began awarding grants to a number of Kansas primary care and mental health safety net providers who were seeking to integrate traditional primary care with mental health and substance use disorder services, categorized as behavioral health care. Studies have shown that people diagnosed with a mental illness lose a median of 10 years of life compared to those without it. Individuals with a serious mental illness (SMI) have higher rates of co-occurring chronic medical conditions, such as high cholesterol, high blood pressure, asthma and diabetes, which can complicate their care and affect the quality of their lives. Care for individuals diagnosed with a mental illness or substance use disorder (SUD) is also much costlier than for those who have no behavioral health diagnosis (Figure 1).
In 2016, the Sunflower Foundation (Sunflower) contracted with the Kansas Health Institute to study the integration efforts of their provider grantees in order to gain an understanding of their successes and challenges in attempting to provide integrated care for their patients.
As a result of the efforts of the grantees (all of which are safety net providers), new service delivery models that integrate traditional primary care with behavioral health care emerged. While the approaches taken by the providers varied, they all share the same goals of improving and streamlining the health of their patients and ultimately reducing costs.
Models of Care
Integrated care models generally fall into three major categories—coordinated care, co-located care, and fully integrated care.
Coordinated care generally involves basic collaboration between the patient’s primary care and mental health providers and typically involves one of the providers referring their patients to another location to receive care. In some cases, the providers may occasionally share information with each other about their shared patients.
In co-located care, both providers are located at the same site but maintain separate office arrangements and treatment plans for their patients or may share some systems and operate somewhat like a team with some face-to-face communication about their shared patients.
With fully integrated care, the primary care and behavioral health providers closely collaborate on treatment planning for their shared patients or may completely integrate their practice for all of their patients, who are cared for by a team of providers who jointly develop and deliver a single treatment plan.
In Kansas, the Sunflower grantees took a variety of approaches to providing integrated care, adopting versions of both the co-location and fully integrated models, with the goal of creating a system that could address all of the physical and behavioral health needs of their patients.
For example, in Sedgwick County, COMCARE, a community mental health center (CMHC), partnered with GraceMed, a federally qualified health center (FQHC), to establish a “mini” FQHC within COMCARE. In Pittsburg, Community Health Center of Southeast Kansas, the largest community health center in Kansas, fully embraced the integrated care model by adding behavioral health professionals to their staff. In Wichita, HealthCore Clinic, which utilizes a team-based approach to create a patient-centered medical home for its patients, hired a behavioral health professional to join their team.
Barriers to Integrated Care
Integrating primary care and behavioral health care is intended to improve outcomes for patients and reduce costs. However, in their efforts to provide integrated care, the Sunflower grantees encountered a range of obstacles or barriers to achieving these goals.
Reimbursement for services
One of the most significant and challenging barriers for the Sunflower grantees was their ability to get reimbursed for the integrated care services they were providing. Unlike Medicare, which allows providers to receive reimbursement for some integrated care services through a small number of approved reimbursement codes, the Sunflower grantees are often not able to obtain payment for the integrated care services they provide to patients covered by KanCare, the Kansas Medicaid program, or by commercial payers (insurers). Although some of the KanCare managed care organizations and other payers sometimes provide payment under limited circumstances to certain types of providers, most of the reimbursement codes available for Medicare patients are not approved for use for KanCare patients and those with private insurance coverage.
For payers, who generally seek to control costs, opening new codes is a policy choice or business decision that is based on balancing additional spending against the potential for measurable improvements that might reduce other costs.
Prospective payment system limitations
The Prospective Payment System (PPS) rate is a fixed payment rate that FQHCs receive for any visit by a Medicare or Medicaid patient. While the Medicare and Medicaid PPS rate methodologies differ, both typically result in a PPS rate for FQHCs that is higher than fee-forservice rates for certain types of services.
While the PPS rate makes FQHCs promising settings for providing integrated care services, certain PPS rate requirements limit reimbursement, including:
FQHCs may bill the PPS rate only when certain types of providers—determined by license levels defined by federal and state governments—deliver services. Some Sunflower grantees reported they are unable to hire or contract with the types of professionals currently eligible for reimbursement at the PPS rate because they are not available in their areas.
Typically, FQHCs may not bill the PPS rate more than once a day, although there are exceptions for separate encounters. Some Sunflower grantees reported there is not a consistent interpretation of when billing for more than one service—for example, a primary medical care visit and a behavioral health intervention—is allowed by the KanCare MCOs. Additional guidance from the state Medicaid agency regarding what kind of behavioral health interventions constitute a “separate encounter” could help remove uncertainty.
Alternative reimbursement
Integrated care models often involve providing services that are not necessarily eligible for reimbursement, but are intended to reduce costs over time in settings other than the integrated clinic itself—for example, reducing the need for hospital admissions or costly long-term care.
Some Sunflower grantees suggested that a “globally funded” reimbursement model or approach would allow them to provide more integrated care services for more patients. Such models in other states include population-based care management fees and shared-savings models, or adaptations of the Accountable Care Organization (ACO) model, which has been implemented in other states using global capitated payments, shared savings and other risk-based methodologies.
While the Kansas MCOs have flexibility under the current KanCare contract to enter into voluntary alternative reimbursement models with providers, the current Medicaid Management and Information System (MMIS) is not designed to routinely accept data from reimbursement models that are not based on currently covered codes. The state’s new MMIS, the Kansas Medicaid Modular System (as planned), will be designed to allow on-system reporting of alternative reimbursement models, which may encourage the MCOs to further explore those options
Facilities and oversight
In addition to limitations on which licensed professionals may bill for select integrated care services, some Sunflower grantees pointed to facility licensure issues potentially affecting integration.
In Kansas, licensure for behavioral health providers is generally more complex than for primary care providers. For example, CMHCs are licensed by the Kansas Department for Aging and Disability Services (KDADS). KDADS also separately licenses substance use disorder (SUD) treatment facilities, which means that CMHCs that seek to provide SUD treatment must be licensed for both. For some Sunflower grantees, this complexity was a significant driver in the decision to use a primary care provider as the base for integrated care.
Options to address this complexity could include reviewing current regulations to increase consistency across existing license types.
Confidentiality and patient records
Existing federal regulations that control the disclosure and use of alcohol and substance use patient records place limitations on who may view the records, how they can be used, and the process for obtaining authorization to disclose them to others.
The Sunflower grantees reported that limitations on a primary care professional’s access to those records sometimes interfere with their efforts.
Grantees who raised concerns about the challenges of shared patient records indicated they have generally found ways to satisfy the confidentiality and privacy concerns with specific types of signed patient releases. However, some stated that the current guidance on the interpretation of the regulations lacks clarity, leading to inconsistent interpretation among providers.
Some of the grantees also noted that the electronic medical record systems they are currently using were not designed to accommodate the entry of additional notes or text into the patient’s record that can be viewed by all members of a patient’s integrated care team.
Culture and workforce
Although the concept of providing integrated care is not new, not all primary care professionals have been trained and may or may not be comfortable working in an integrated care environment.
In addition to the challenges related to attracting health professionals to serve patients with complex health needs, some Sunflower grantees noted that it is critical that all health professionals working in an integrated care setting embrace the model and recognize the need for behavioral health services for their patients in the absence of a crisis.
The grantees suggested that providing opportunities for medical and health professions students to experience working in an integrated care setting could ensure a primary care workforce eager to partner with behavioral health professionals to implement integrated care models for their shared patients.
Future Solutions
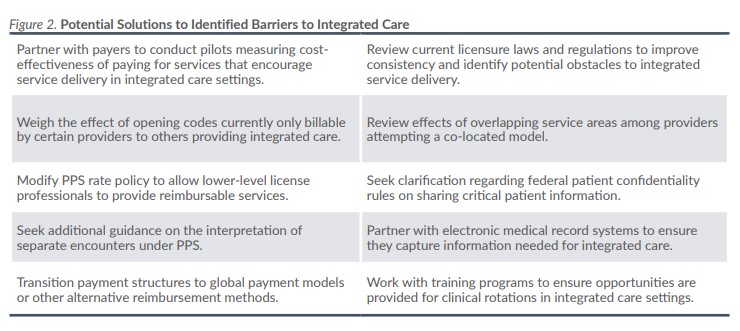
With a vision of improving health outcomes and reducing long-term costs, the Sunflower Foundation grantees have found innovative and creative ways to provide integrated primary medical and behavioral health care for their patients, but also have encountered various barriers and challenges. Figure 2 includes a list of potential solutions to many of the identified barriers, but a convening of stakeholders could likely identify other solutions. The Sunflower grantees said they would welcome the opportunity to work with federal and state policymakers to find ways to reduce or eliminate the barriers they have encountered, and possibly encourage additional providers to adopt an integrated care approach for their patients.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.