Kansas and Current CCBHC Operations
While Kansas was not in the first wave of CCBHC demonstration states, it was the first state to pass legislation that identified the CCBHC model as a solution to the mental health and substance use crisis. Established through Senate Substitute for House Bill 2208 in 2021, CCBHCs in Kansas are certified by the Kansas Department for Aging and Disability Services (KDADS).
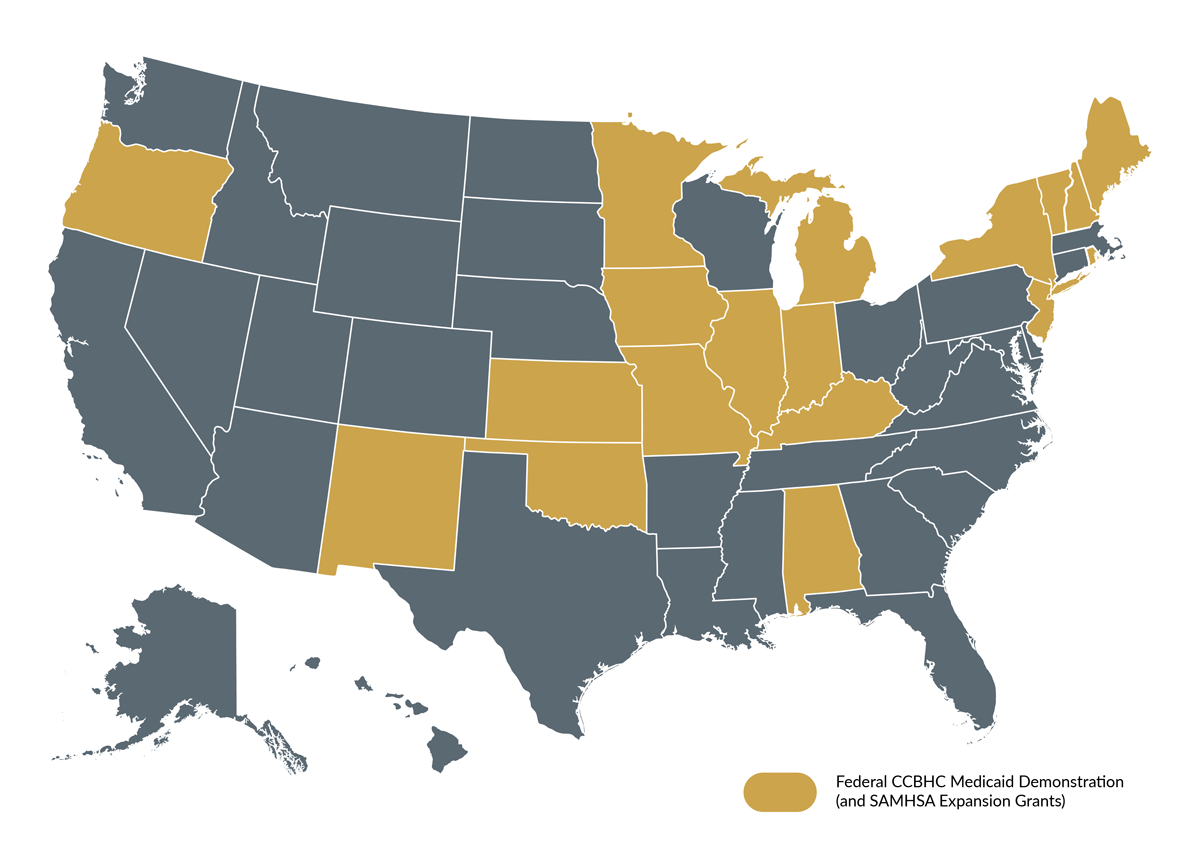
The initial push for CCBHCs in Kansas was supported by federal funding opportunities and grants aimed at expanding access to mental health care. In 2022, Kansas was awarded a federal planning grant from SAMHSA to support the development and expansion of the model. The state has transitioned all 26 existing community mental health centers covering the 105 Kansas counties into CCBHCs. As of now, CCBHC certification is limited to community mental health centers. However, with the passage of House Bill 2784 in 2024, any community mental health center or qualified nonprofit provider meeting the criteria will be eligible for certification beginning on Feb. 1, 2027.
As Kansas transitions into the Medicaid demonstration program, organizations such as the Bert Nash Community Mental Health Center in Douglas County illustrate how this model is able to reshape the delivery of care. Patrick Schmitz, CEO of Bert Nash, explained, “As a community mental health center, we are responsible for the behavioral health care of this community and making sure that [individuals] have access to [care] regardless of the level of illness that they have and their financial status.”
The CCBHC framework has enabled Bert Nash to significantly expand their services. The center is now offering over 40 programs that include nutritional therapy, school-based care, housing support, substance abuse training and psychiatric advisement. This model allows for timely access to care based on the severity of need: triage categories are arranged by crisis, urgent and routine, which allows the center to provide same-day support to those in crisis. Schmitz states that if clients need attention for three hours the same day, the CCBHC framework allows this to be possible. This is a major shift from the pre-CCBHC approach where initial assessments could take up to 30 days or more.
In addition to more positive clinical outcomes, the implementation of the CCBHC framework has had positive impacts on staff retention. Schmitz reiterated that keeping staff is critical to the retention and development of skills. Through the CCBHC model, temporary training can be transformed into long-term career skillsets for behavioral health providers.