Section 1332 of the Affordable Care Act (ACA) allows individual states to develop their own approaches to health reform.
A state’s waiver application must show its plan will meet the comprehensive coverage, affordability, coverage for comparable number of residents, and budget neutrality requirements.
States that receive waivers may become eligible for federal dollars to help implement their waiver plans.
While no state has submitted a waiver application yet, at least eight states are considering doing so: Arkansas, California, Hawaii, Massachusetts, Minnesota, New Mexico, Rhode Island and Vermont.
Introduction
For Kansas and other states that have been opposed to the content and philosophy of the Affordable Care Act (ACA), a section of the law provides an opportunity to opt out of some of its key requirements beginning in 2017. The federal law has significantly impacted health insurance markets and premium costs in all states. Section 1332 of the law could be the catalyst for individual states to develop and implement state-specific approaches to health reform and coverage for their citizens. However, substantial state capacity and commitment will be required to put together a credible plan and meet all the waiver application requirements.
Alternative Strategies Under Section 1332, which is titled Waiver for State Innovation, states may apply to the secretary of the U.S. Department of Health and Human Services (HHS) for a waiver to implement alternative strategies to provide their citizens with access to affordable health care.
The concept for the Section 1332 waiver began in 2007 with the development of the Healthy Americans Act, in which Senator Ron Wyden (D-OR) raised the idea of providing a waiver for states to develop alternative health reform plans. The concept of Wyden’s waiver for state innovation was included in the final version of the Healthy Americans Act, which never passed but was ultimately merged into the health reform bill that became the basis of the ACA.
With a Section 1332 waiver, states may opt out of any or all of the following elements of the ACA:
Certification of qualified health plans or requirements for essential health benefits
Premium tax credits and cost-sharing subsidies provided for some low-income individuals and families who purchase health plans through a health insurance marketplace
Delivery of benefits through a health insurance marketplace
Employer-shared responsibility mandate
Individual mandate to maintain minimum essential coverage.
A Section 1332 waiver—which can begin on or after January 1, 2017—would be in effect for five years and may be extended beyond that. If a state’s waiver makes its citizens ineligible for premium tax credits, cost-sharing subsidies or small business tax credits, the state may receive an aggregate amount of such funds to implement its waiver plan.
Waiver Requirements
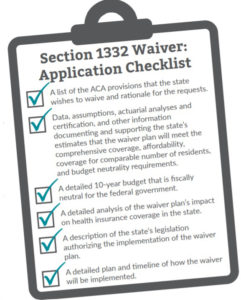
A state’s waiver application must demonstrate that its proposed waiver plan will:
Provide comprehensive coverage that is comparable to the coverage offered through the ACA
Ensure affordability by providing coverage and cost-sharing protection against excessive out-of-pocket spending
Provide coverage to at least a comparable number of residents as the ACA
Ensure the waiver plan will not increase the federal deficit.
State-Based Reform
Even before the ACA was enacted in 2010, state policymakers were interested in finding ways to increase access to health care and health insurance coverage in order to improve the health of their citizens. However, these efforts were often made more difficult by the financial limitations of state budgets. A Section 1332 waiver—and the funds it could provide— may allow a state to modify its Medicaid program, Children’s Health Insurance Program (CHIP) and/or private health insurance market in order to implement health care programs that better reflect the goals, demographics and political culture of the state.
Although HHS has provided little information to-date regarding what ideas or innovations they are willing to approve, health policy experts and some state officials have started to generate ideas of how states might structure a Section 1332 waiver plan, including:
Preserving or enhancing the employer-sponsored health insurance market and finding ways to make coverage more affordable for both employers and employees
Providing various levels of cost-sharing and encouraging personal responsibility for individuals based on income
Making coverage more seamless for families with members enrolled in Medicaid/CHIP, employer sponsored coverage or individual coverage
Encouraging the development and growth of commercial market alternatives to the federal marketplace
Standardizing and streamlining eligibility and enrollment processes, making it easier and more attractive for consumers to apply for different types of coverage
Maintaining continuity of care when individuals and families experience changes in income, family size or employment
Structuring health coverage to provide incentives for healthy behaviors.
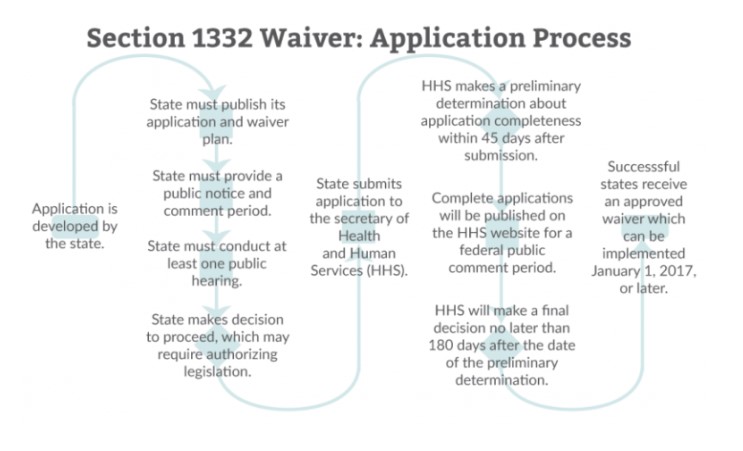
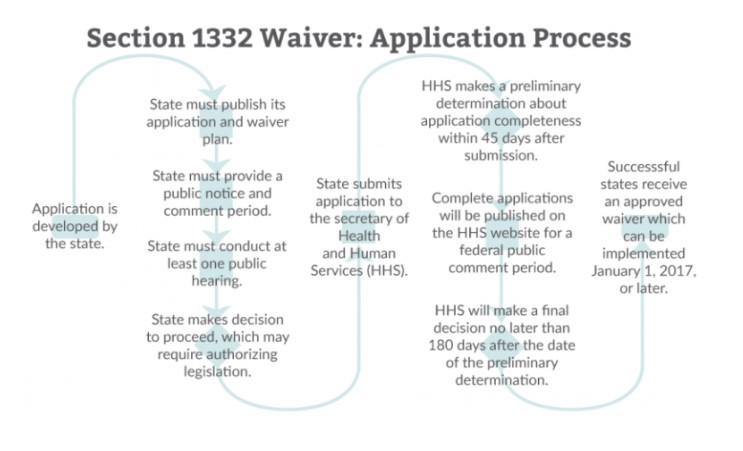
1332 Waiver Application Process
Prior to submitting an application for a Section 1332 waiver, a state must publish its application and waiver plan, provide a public notice and comment period, and conduct public hearings to allow input and written comments regarding the application. Authorizing legislation may also need to be enacted.
Within 45 days after submitting the application to the secretary of HHS, a preliminary determination will be made as to its completeness. Complete applications will then be published on the HHS website for a federal public comment period. A final decision regarding the waiver will be issued no later than 180 days after the date of the preliminary determination.
An approved Section 1332 waiver will not change or impact a state’s authority under any existing Medicaid, CHIP or Medicare waivers. However, a state may apply for such waivers as a part of a coordinated application process established by the HHS secretary for a Section 1332 waiver.
Potential Challenges
While a Section 1332 waiver has the potential to allow states more autonomy in health reform, the time and effort needed to develop a plan that meets all the technical requirement of the federal legislation, then to enact state legislation would be significant. In addition to ensuring its plan meets all the requirements established under the federal law and the regulations issued by HHS, states also will likely encounter concern or opposition from interested parties who may object to the perceived loss of certain ACA protections or benefits, or who may question how a state will implement and administer the financial, regulatory and health care elements of the state’s plan.
The presidential election in November 2016 adds an element of uncertainty for states that choose to develop and submit a Section 1332 waiver application during 2016 for implementation in 2017. If a Republican president is elected, there is potential for repeal or significant modifications to the ACA. In that case, the waiver option may no longer be available to states or, in the alternative, could become more comprehensive and allow states additional freedom to explore state alternatives. With the election of a Democratic president, states may find themselves faced with new rules and requirements for waiver plans and the application process. States also may find that a new Democratic administration has a very different view of the value of waivers and may be more or less willing to approve waivers that attempt to test the boundaries of the waiver option and what the new administration is willing to approve.
Section 1332 Waiver Activity
A number of states—including New Mexico, Rhode Island, California and Massachusetts—have already indicated their interest in submitting a Section 1332 waiver application and have enacted or introduced legislation, established advisory boards or task forces, or held public meetings to establish policy goals for a waiver. A small number of states have made greater progress in their waiver planning, including:
Minnesota
According to the 2017 Innovation Waiver Progress Report from the Minnesota Department of Human Services Health Care Administration, the state has identified three areas of focus to provide residents with a seamless coverage experience. The first focus area will use both a Section 1332 waiver and a Section 1115 waiver to align eligibility and enrollment requirements across insurance affordability programs, which provide coverage for lower-income individuals in the state. The second focus area will create multipayer alignment in payment and delivery reform across insurance affordability programs that will realign incentives so providers are working toward the same goals of quality and efficiency. The third focus area will align coverage and contracting requirements between public and private insurance programs to improve care and reduce coverage disruption for consumers.
Arkansas
Governor Asa Hutchinson has indicated an interest in moving beyond the state’s use of its Section 1115 waiver—which authorized the state’s “private option” approach to expanding Medicaid—by designing a new marketplace for health care and insurance for 2017. The Arkansas legislature has approved funding for the private option through the end of 2016 and has formed a task force to develop recommendations for health care reform. Hutchinson has indicated that a combination of Section 1115 and Section 1332 waivers could present an opportunity to build on the existing private option.
Vermont
Vermont worked for four years to establish a state based, single-payer plan, but ultimately determined the potential cost and financing challenges were too great to overcome. The state has indicated its intent to pursue a Section 1332 waiver in order to take advantage of the federal dollars that may become available. The plan combines the additional federal funding with state funding to provide a publicly financed gold-level benefit plan to all of its residents. Vermont’s single-payer approach also would include its Medicaid and CHIP programs, which would be supplemented to meet the “gold-level” benefit standard.
Hawaii
Hawaii intends to submit a Section 1332 waiver application that will allow it to preserve its employer mandate, which has been in place since 1974 and has reduced its uninsured rate to less than 10 percent. The state has published its waiver plan—which proposes to improve coverage, health care delivery, payment and wellness in the state—to allow for public review and comment, as required under the Section 1332 waiver application process.
Conclusion
The Section 1332 State Innovation Waiver provides an opportunity for states, like Kansas, to create a health care and coverage system that fits the unique demographics and health care needs of residents and reflects the political ideals of policymakers and other stakeholders. However, substantial state capacity and commitment will be required to put together a credible plan and meet all the waiver application requirements. KHI will continue to monitor the progress of states exploring Section 1332 waivers.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.