
Introduction
On January 14, 2019, the first day of the 2019 Kansas legislative session, Sen. Laura Kelly (D-Topeka) will be sworn in as the 48th governor of Kansas. The 2019 legislative session will mark the first year of a two-year cycle.



On January 14, 2019, the first day of the 2019 Kansas legislative session, Sen. Laura Kelly (D-Topeka) will be sworn in as the 48th governor of Kansas. The 2019 legislative session will mark the first year of a two-year cycle.
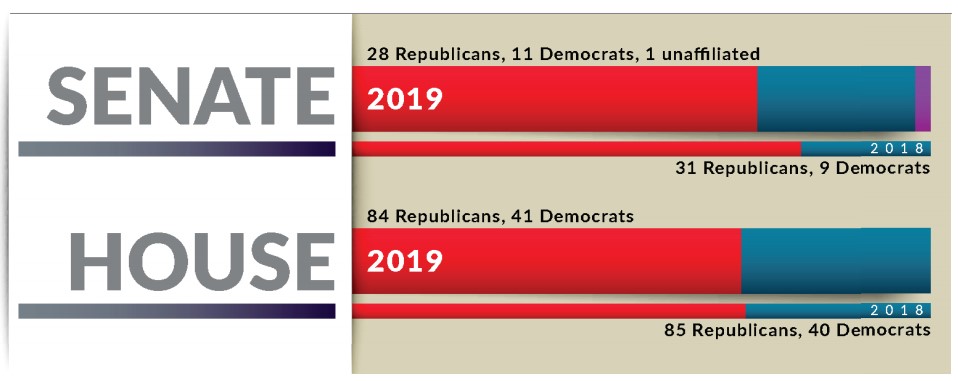
As a result of the 2018 elections, there will be 29 new House members and three new senators in 2019. On the Senate side, Rep. Vic Miller (D-Topeka) was selected to complete Sen. Kelly’s term; Mary Ware, who is not currently serving in the Legislature, was selected to complete the term of Sen. Lynn Rogers, who will serve as Lieutenant Governor beginning in 2019; and Assistant Secretary of State Eric Rucker was selected to complete the term of Sen. Vicki Schmidt, who was elected to serve as Insurance Commissioner.
Freda Warfield will be replacing Rep. Miller in the House. Republicans continue to hold majorities in both chambers with 28 Republicans, 11 Democrats and one unaffiliated in the Senate and 84 Republicans and 41 Democrats in the House.
Between January 14 and the end of the session — generally in early May — the Legislature will have numerous issues to consider. While producing a state budget is the only constitutionally required act, lawmakers likely will consider action on many significant health policy issues.
In 2019, legislators likely will have an opportunity to consider Medicaid expansion under the provisions of the Affordable Care Act (ACA). Gov.-elect Kelly stated repeatedly throughout her campaign that expansion would be a high priority in her first year of office, but there are opponents to expansion among the members of the Legislature. The Governor’s Substance Use Disorders (SUD) Task Force, the Mental Health Task Force, and the Child Welfare System Task Force all included recommendations for Medicaid expansion in their 2018 reports to the Legislature.
A KHI report projected that approximately 145,000 Kansans — including 95,000 adults — would newly enroll in KanCare, the state’s comprehensive managed care program that combines Medicaid and the Children’s Health Insurance Program (CHIP), if the state expands Medicaid up to 138 percent of the federal poverty level ($34,638 for a family of four in 2018) as provided under the ACA.
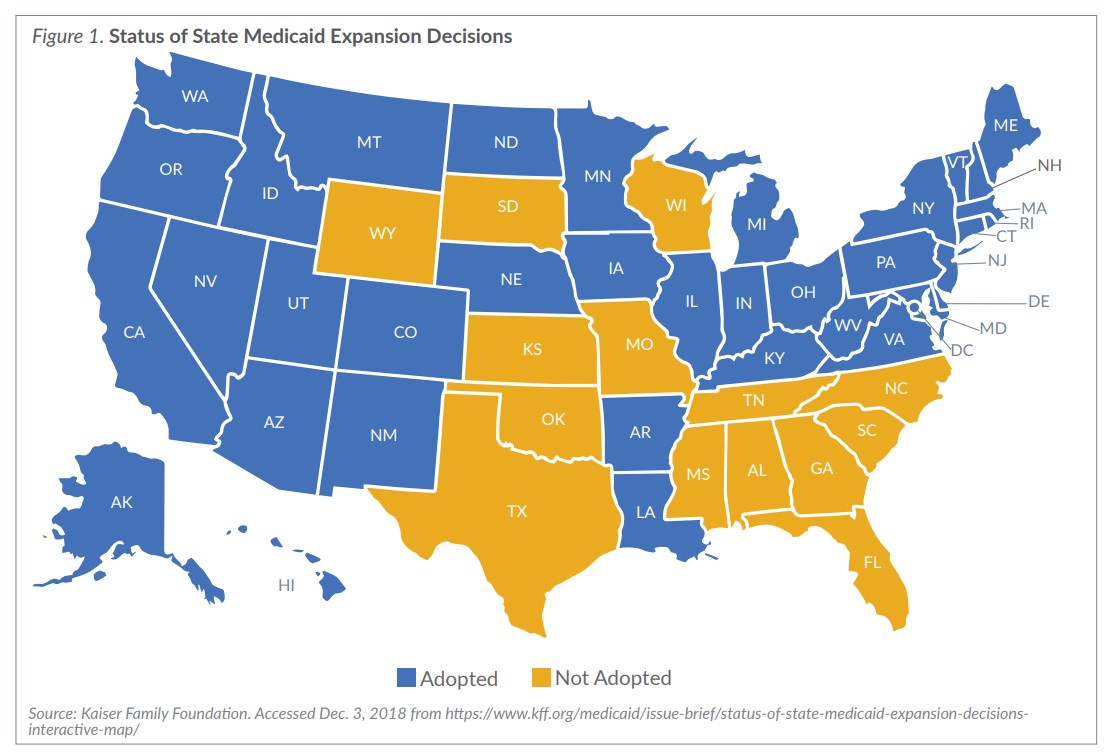
To date, 36 states and the District of Columbia have expanded Medicaid under the ACA (Figure 1), including the states of Utah, Idaho and Nebraska, where voters approved ballot measures for expansion in November 2018. Eight expansion states have adopted “non-traditional” approaches to Medicaid expansion through Section 1115 waivers, which have allowed them to establish various types of programs or requirements for their enrollees including:
The 2017 Kansas Legislature, with Republicans in the majority in both the House and Senate, passed a bill to expand Medicaid that was vetoed by Gov. Sam Brownback. At the time of his veto, Gov. Brownback stated one of his objections to expansion was uncertainty about the efforts of Congress to repeal, replace or modify the ACA. In 2017, both the U.S. House and the U.S. Senate proposed and voted on bills to repeal or modify various provisions of the ACA, including the Medicaid expansion option. In 2018, Congress took no formal action on the ACA; however, President Donald Trump and his administration took several actions designed to give states more flexibility in the design and operation of their Medicaid programs using Section 1115 waivers. On December 14, 2018, Judge Reed O’Connor, a federal district court judge in Texas, issued an opinion declaring that the entire ACA is invalid, including all provisions related to the Medicaid program. Legal experts on both sides of the case anticipate an appeal of the case, which may ultimately land with the U.S. Supreme Court, and the ACA remains in effect for now.
Beginning on January 1, 2019, the three managed care organizations (MCOs) that will be providing services to KanCare beneficiaries will be Sunflower State Health Plan, Inc.; United Healthcare, Midwest Inc.; and Aetna Better Health of Kansas, Inc. Both Sunflower and United Healthcare, which have served as KanCare MCOs since 2013, received contract renewals in June 2018. Aetna is replacing the third original MCO, Amerigroup Kansas.
At the conclusion of the meeting of the Robert G. (Bob) Bethell Joint Committee on Home and Community Based Services and KanCare Oversight on November 8-9, 2018, legislators discussed and voted to approve several recommendations to be made to the full Legislature, including:
The Mental Health Task Force (MHTF), established by the Legislature in 2017 and reauthorized in 2018, was charged with developing an implementation plan by January 14, 2019, for the 26 recommendations in their January 2018 report (bit.ly/2Scj2TG).

For one of the 2018 MHTF recommendations, legislators requested that the Kansas Department for Aging and Disability Services (KDADS) contract with KHI to conduct a study estimating the number of psychiatric inpatient beds needed statewide. The estimate is to be included in the 2019 report of the MHTF and is likely to be discussed during the 2019 legislative session. On November 20, 2018, KDADS released a request for proposals to increase regional inpatient treatment capacity.
The Governor’s Substance Use Disorders (SUD) Task Force, which was established by Gov. Jeff Colyer in March 2018, convened from April 2018 to August 2018 and released its report on September 1, 2018. The report included 34 high-priority recommendations (bit.ly/2GIoYCS) focused on prevention, provider education, treatment and recovery, law enforcement, and neonatal-abstinence syndrome (NAS). The recommendations also included funding and changes in utilization for K-TRACS, the Kansas drug monitoring program, which would require legislative action, including:
On June 1, 2018, the Kansas Department of Health and Environment (KDHE) began requiring prior authorization before opioid products could be prescribed for pain management for all KanCare enrollees. Prior authorization — a process through which a prescription must be pre-approved by an insurer prior to being dispensed — now is required for both short- and long-acting opioids. Exemptions to the prior authorization process apply for certain individuals (e.g., patients with cancer). Other policies to curb opioid abuse may be considered by the Legislature in the 2019 session, including recommendations put forward by the SUD Task Force.
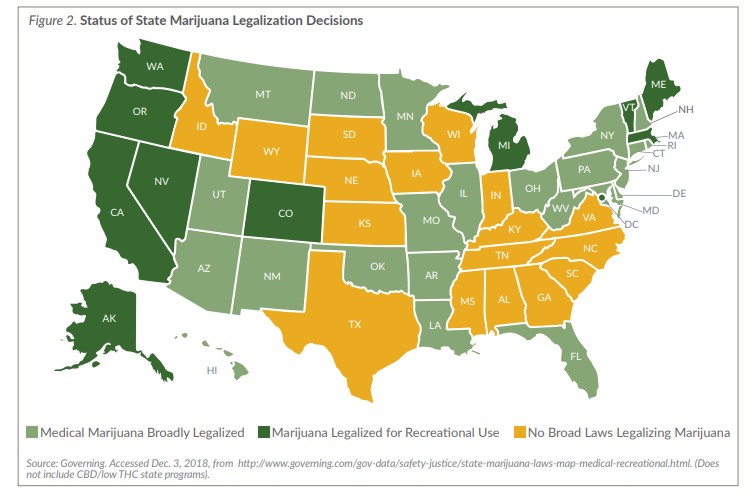
As of November 2018, 33 states and the District of Columbia have passed laws legalizing marijuana in some form (Figure 2, page 5). The District of Columbia and 10 states — Alaska, California, Colorado, Maine, Massachusetts, Michigan, Nevada, Oregon, Vermont and Washington — have adopted laws legalizing marijuana for recreational use, while 23 other states allow limited use of medical marijuana under certain circumstances.
In 2018, Kansas legislators updated the substances included in Schedules I, II and III of the Uniform Controlled Substances Act and an amendment offered during House debate on the bill to allow medical marijuana use in the state was considered but ultimately rejected on a vote of 54-69.

With the approval of medical marijuana by Missouri voters in November 2018, Kansas is now bordered on three sides by states that have legalized either recreational or medical marijuana use. Gov.-elect Kelly has stated she supports legalization of medical marijuana provided it is well-regulated, and although legalization is opposed by some legislators, it appears some opponents may be open to considering a bill.
In November 2018, the Centers for Medicare and Medicaid Services (CMS) released new guidance related to state innovation waiver applications under Section 1332 of the ACA that could help Kansas legislators implement policies to stabilize the Kansas individual insurance market. The guidance describes types of programs or policies that may be implemented under an innovation waiver, such as using ACA premium tax credits to assist consumers with purchasing health plans based on their needs, establishing subsidy programs, providing a wider range of health care options, and establishing risk stabilization programs, such as state-based reinsurance programs. While states still are required to satisfy certain requirements or “guardrails” stated in the ACA, CMS is encouraging states to submit proposals so it may assess their feasibility under the provisions of the law.
In June and August 2018, the Trump administration finalized two major regulations intended to expand insurance options available to employers and consumers — one expanded the use of association health plans (AHP) and the other lengthened the term of short-term, limited duration insurance (STLDI). However, some provisions of the new regulations cannot be implemented in Kansas because they are prohibited under Kansas law. The Kansas Chamber of Commerce, and perhaps other organizations, are interested in amending Kansas law to comply with the new federal rules and likely will introduce legislation early in the session.
The Child Welfare System Task Force, created by the Legislature in 2017, was charged with convening working groups to study the administration of child welfare by the Kansas Department for Children and Families (DCF), and study protective services, family preservation, reintegration, foster care and permanency placement. After numerous meetings beginning in August 2017, the task force adopted 24 recommendations (bit.ly/2EGiXEF) for submission to the Legislature. The top priority recommendations that would likely require action by legislators include:

In 2018, legislators passed the Kansas Pharmacy Patients Fair Practices Act, which allows pharmacies and pharmacists to provide insured consumers with information regarding the amount of the covered person’s share of costs for prescription drugs. It specifically prohibits pharmacy benefit managers (PBMs) from prohibiting pharmacists from discussing or selling a more affordable alternative to the consumer.
In the absence of congressional action addressing the high cost of prescription drugs, Kansas legislators may want to look at actions taken by legislators across the country to address drug costs, including importing drugs from Canada, setting rates, purchasing in volume, requiring cost transparency and prohibiting price-gouging.
During the 2018 legislative session, an amendment to the Kansas Constitution was introduced to reduce the sales tax on food in Kansas. Kansas is among the states with the highest rates of food taxation. Though the Senate Committee on Assessment and Taxation heard the proposed revision, the resolution died in committee. During the 2018 general election, gubernatorial candidates and several legislative candidates weighed in on the issue of sales taxes on food. While other demands on state funds, including K-12 education funding, may present a barrier to this initiative, the 2019 Legislature may see new activity on this issue.
Senate Substitute for House Bill (HB) 2600, enacted by the Legislature in 2018, established the Palliative Care and Quality of Life Interdisciplinary Advisory Council. The council, which is charged with developing recommendations and advising KDHE on matters related to the establishment, maintenance, operation and evaluation of palliative care initiatives in the state, held its first meeting on November 30, 2018. Although the council is not scheduled to meet again until April 26, 2019, legislators may be interested in taking another look at additional legislation related to this issue or the council’s charge.
One in three rural Kansans lacks adequate access to the internet, which supports the health of communities by enabling communications and providing access to resources for schools, doctors, emergency services and other critical sectors of the community. In 2018, legislators established the Statewide Broadband Expansion Planning Task Force, which is charged with a number of tasks, including developing criteria for the creation of a statewide map for defining and evaluating the broadband needs of Kansas citizens, businesses, industries, institutions and organizations and identifying risks and constraints associated with a statewide broadband expansion program. The task force, co-chaired by Sen. Rob Olson and Rep. Joe Seiwert, will be meeting for the first time on January 11, 2019, and may generate some legislative action later in the session.

A bill to license mid-level dental therapists to address shortages of dental providers in some parts of the state was introduced in the Senate Public Health and Welfare Committee early in the 2018 session. While an amended version of the bill, which was supported by the Kansas Dental Association, passed the Senate, it failed to receive a vote in the House Health and Human Services Committee. Mid-level dental therapist legislation has been consistently introduced and considered by the Legislature for many years and the Kansas Dental Hygienists Association has indicated it will reintroduce in 2019 the bill that passed out of the Senate last year.
State Budget
Governor-elect Kelly will release her budget in the weeks following her inauguration in January 2019. In November, the Consensus Estimating Group revised its State General Fund (SGF) revenue estimates.
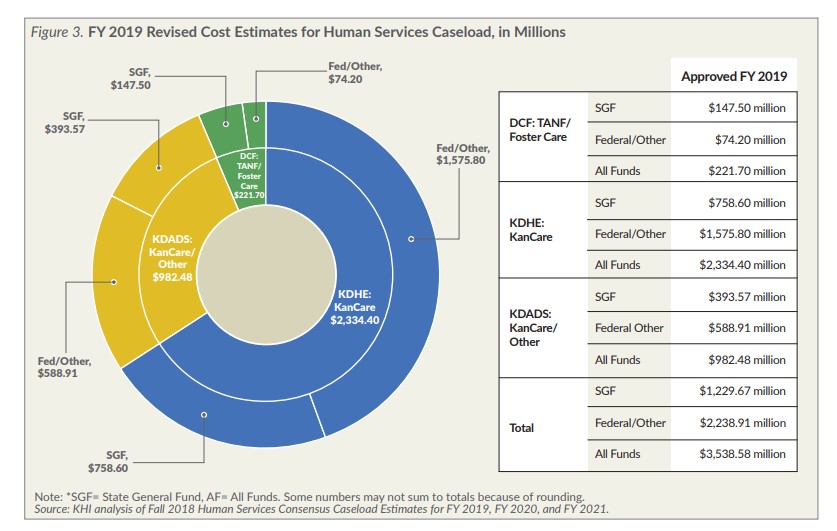
Even after incorporating a $54.6 million SGF increase in Human Services Caseloads estimates (Figure 3), the projected SGF ending balance for Fiscal Year 2019 was raised to $905 million, or 12.6 percent of state expenditures, well above the statutorily required 7.5 percent.
The estimated ending balance does not include potential policy changes that could be considered by the 2019 Legislature, including adding an inflation factor to K-12 education spending or expanding KanCare. It also does not include nearly $105 million in newly requested SGF from state agencies to enhance or supplement their FY 2019 budgets. Examples include $1.1 million for the Department for Children and Families to add child welfare workers, $2.2 million to improve Medicaid Eligibility Clearinghouse operations, $19.3 million to enhance operations and staffing at Larned State Hospital and Osawatomie State Hospital, $12.5 million to begin a five year-process to replace patient management systems at the four state hospitals, and $7.8 million to increase funding to Community Mental Health Centers. The SGF total for all agencies’ requested enhancements and supplementals in FY 2020 and 2021 would climb to $505 million and $655 million, respectively.
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.