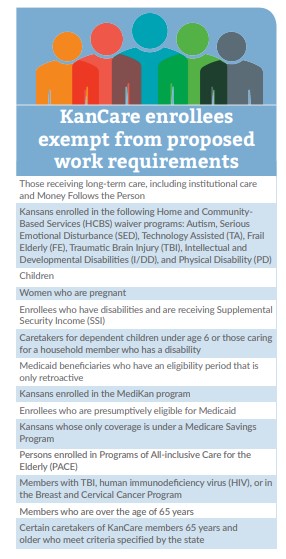
A poll released on May 8 by the American Cancer Society’s Cancer Action Network and the American Heart Association found that 68 percent of Kansans surveyed support expansion. KHI has estimated that approximately 152,000 Kansans—including 98,000 adults—would newly enroll in KanCare if the state expanded Medicaid up to 138 percent of the federal poverty level, as provided under the ACA.
During 2017, both the U.S. House of Representatives and U.S. Senate proposed and voted on a handful of bills to repeal or modify various provisions of the ACA, including Medicaid funding and the expansion option. However, no bill has yet passed. In 2018, GOP leadership likely will resume their efforts. Despite this uncertainty, expansion advocates in Kansas have indicated they intend to pursue expansion again in 2018.
Child Welfare System Task Force
House Substitute for Senate Bill (SB) 126, enacted during the 2017 session, directed the secretary of the Kansas Department for Children and Families (DCF) to establish a Child Welfare System Task Force, including several working groups, to study the child welfare system in the state. The 20-member task force, chaired by Sen. Vicki Schmidt, includes vice chair Rep. Steve Alford, Senators Barbara Bollier and Laura Kelly and Representatives Linda Gallagher and Jarrod Ousley. Other members include individuals representing the judicial branch, law enforcement, social welfare, child advocates, DCF officials and foster care contractors.
The Task Force—charged with studying the administration of child welfare by DCF, protective services, family preservation, reintegration, foster care and permanency placement—began meeting in August and will submit to the Legislature a preliminary progress report by January 8, 2018, and a final report on or before January 14, 2019. The report is expected to recommend changes to current laws, rules and regulations, and child welfare system processes that will result in improved safety and well-being for children in the Kansas child welfare system.
In addition to reviewing the initial findings of the task force, legislators also will begin working with the newly appointed secretary of DCF, Gina Meier-Hummel, who is a member of the Task Force. She was nominated to fill the role of secretary by Lt. Gov. Jeff Colyer on November 21 and started work with DCF on December 1 following the retirement of former secretary Phyllis Gilmore.
Behavioral Health/Osawatomie State Hospital
Mental Health Task Force
The budget passed by the 2017 Legislature included a proviso directing KDADS to establish a task force to review the behavioral health system in Kansas. Comprised of 11 members, the Mental Health Task Force was charged with assessing the strengths and weaknesses of the state’s current behavioral health system and making recommendations for improvements in a report due to the Legislature by January 8, 2018. The recommendations are expected to include a strategy focused on the most effective ways to deliver services for individuals of all ages, the availability of crisis stabilization centers, the maximization of federal and other funding sources for services, the certification of Osawatomie State Hospital (OSH), and options related to privatizing services.