Political Landscape
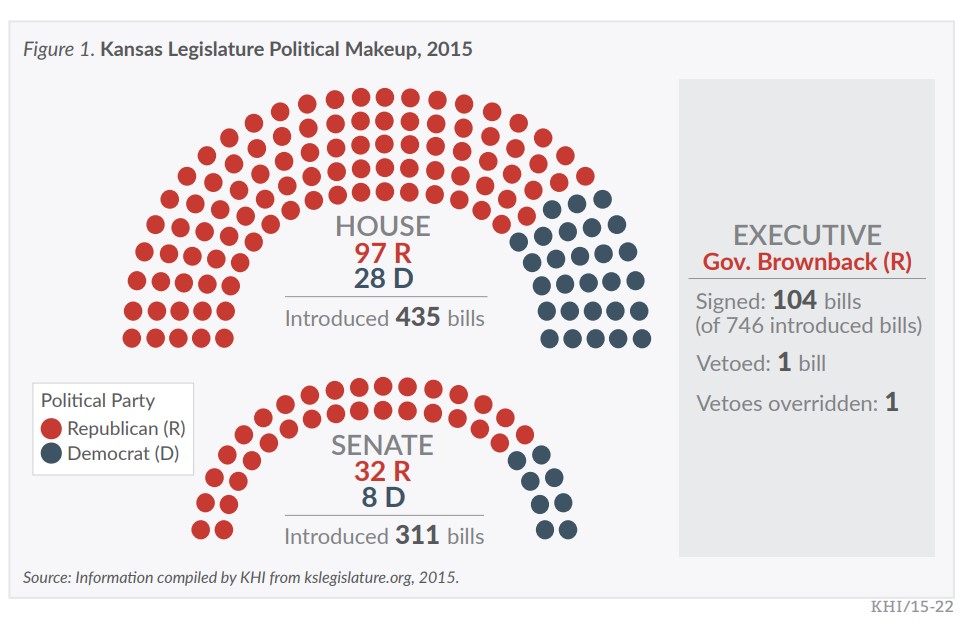
Following the November 2014 elections, Republicans held supermajorities in both the Senate and House. Conservative Republican Governor Sam Brownback was re-elected, promising to continue his signature income tax plan and maintain his focus on economic growth, K-12 education funding, and reforming the public employees’ retirement system.
Overview
Much of the media attention during the 2015 session focused on fiscal issues following the implications of the 2012 tax cuts signed into law by Governor Brownback, which represented the largest tax cut in Kansas history. Shortfalls in tax revenue through fiscal year (FY) 2015 required Governor Brownback to implement cuts in the approved budget before the Legislature returned in January 2015. The 2015 Legislature adopted a budget early in the session that accepted current-year reductions and replaced the K-12 education funding formula with fixed, inflation-adjusted amounts for each school district, or block grants. The final weeks of the session saw legislators gridlocked over tax policy in order to fill the remaining $400 million gap between 2016 revenue estimates and the $6.2 billion budget.
The session ended after a record 113 days, with the Legislature passing a bill that largely closed the budget gap by raising state sales tax from 6.15 to 6.5 percent, raising cigarette taxes by 50 cents per pack, creating a new tax of 20 cents/mL on e-cigarette fluid, and eliminating a number of income tax deductions. The budget bill won some additional votes by eliminating income taxes for the poorest Kansans, though a proposal to lower the food sales tax did not make it into the final bill.
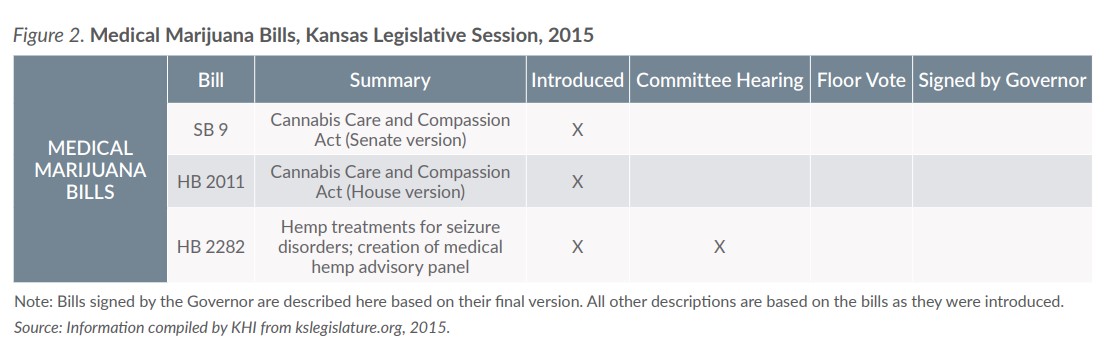
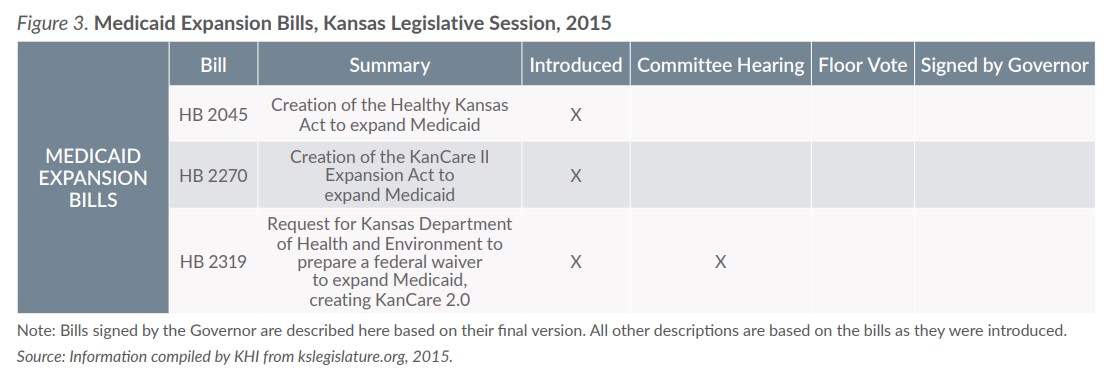
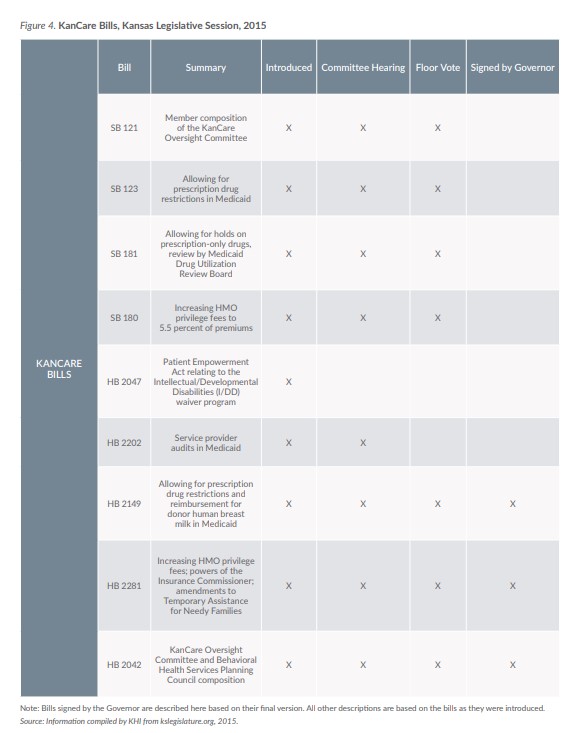
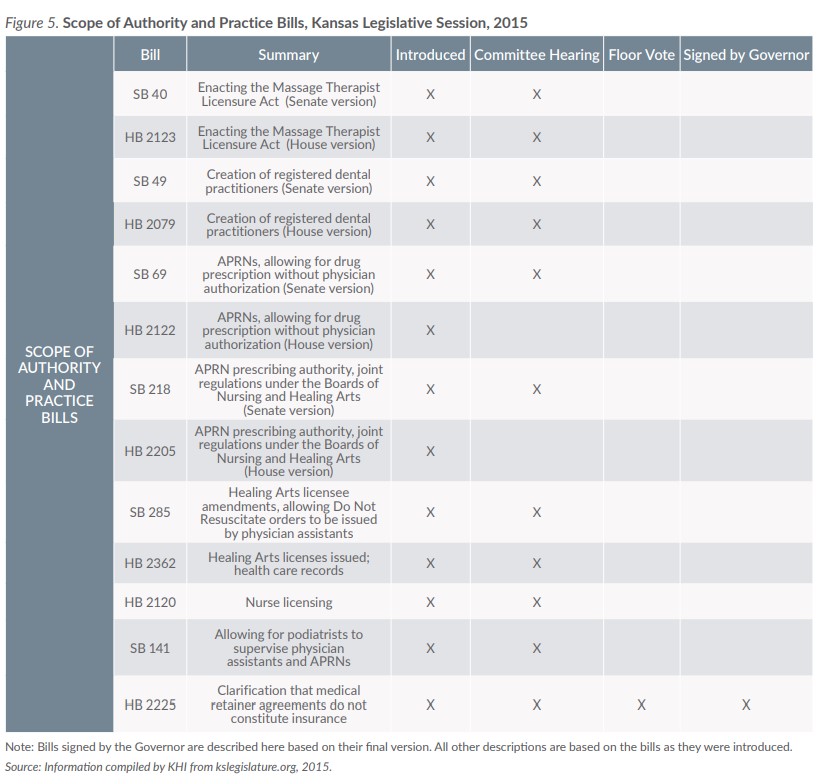
Health policy bills were featured prominently in legislative discussions during the 2015 session, both as stand-alone issues and tied with debates over the budget. The key themes in these bills are likely to return in future sessions.