Disabled population
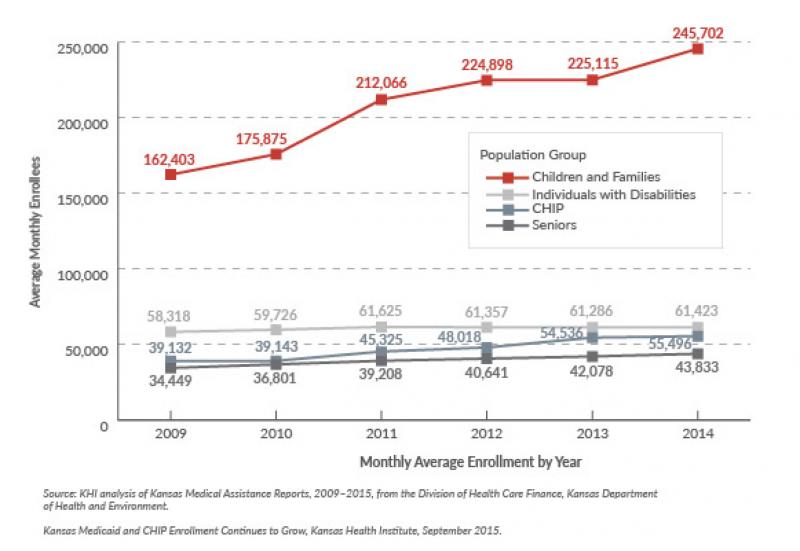
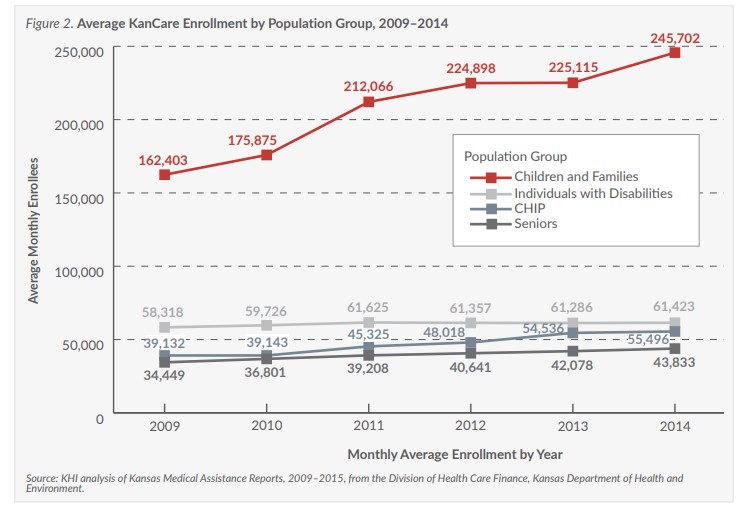
Enrollment was essentially flat (61,286 in 2013 to 61,423 in 2014) for individuals with disabilities during the second year of KanCare. Annual enrollment growth for individuals with disabilities ranged from -0.4 to 3.2 percent between 2009 and 2014.
Seniors
Low-income individuals age 65 or older are eligible for coverage under both Medicaid and Medicare (the federal health insurance program for this age group). This eligibility group grew by 4.2 percent (from 42,078 in 2013 to 43,833 in 2014)—falling within the historical growth trends, which ranged from 3.5 to 6.8 percent between 2009 and 2013.
Policy Impacts
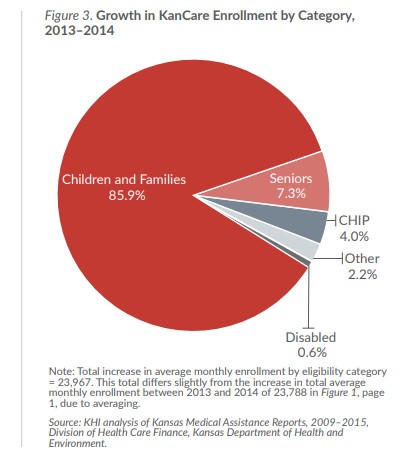
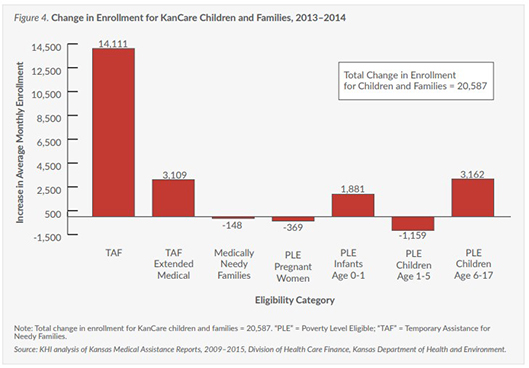
Enrollment growth in KanCare during 2014 is notable for the increases in Medicaid children and family eligibility groups.
The unprecedented jump in TAF, TAF Extended Medical and low-income children enrollment could be attributed to policy changes related to the implementation of the Kansas Eligibility and Enforcement System (KEES). KEES is a computer system designed to replace the existing state system used to keep track of who is eligible for Medicaid and other assistance programs.
KEES allows applicants to submit information electronically to the state for review. KEES also will match information provided with other state and federal databases to help prevent inaccurate information and automate eligibility decisions for medical assistance programs.
Kansas Medicaid policy requires an annual review of eligibility for KanCare. However, all medical assistance eligibility reviews were suspended from October 2013 to March 2014 to temporarily relieve state agency workload during the transition to new policies under the Affordable Care Act (ACA) and the planned implementation of KEES. During this time, KanCare eligibility continued without the required review of case information.
Under normal circumstances, the state agency would collect and update members’ information (such as income and household size) to determine if KanCare eligibility still exists. However, it is unclear how much of a role the implementation of KEES actually played in the observed enrollment increase.
Changes in eligibility rules for cash assistance through TAF could also play a role in changing enrollment in Medicaid. Kansas reduced the lifetime limit for cash assistance from 60 to 48 months as of November 2012 (and has since reduced the limit to 36 months, effective July 2015).
Kansas also raised the requirement to demonstrate job searches or training as a condition of receiving cash assistance. The eligibility changes for cash assistance might be expected to lead to a decrease in enrollment for the TAF group, and an increase in the TAF Extended Medical group.
As more people run out of cash assistance, they could continue receiving extended medical benefits during the four months following the end of cash assistance. The number of people on extended medical should decrease over time as the cash assistance population reaches a lower level. However, the number of children eligible for Medicaid (because of their family income) could continue to grow as a population in Medicaid, even after cash assistance runs out for the family.
Between 2013 and 2014, enrollment of low-income children age 1–5 in Medicaid decreased by 2.1 percent, while enrollment of low-income children age 6–17 in Medicaid increased by 4.4 percent. Historically, enrollment for both of these age groups has grown at about the same rate.
One possible explanation could come from changes in eligibility rules because of the ACA, which required moving some children who were eligible for CHIP to Medicaid starting in January 2014. This change affected children age 6–17 from 99 to 113 percent of the federal poverty level (FPL).
Prior to January 2014, children between 99 and 113 percent of FPL were covered under CHIP. That would suggest growth in Medicaid enrollment for children age 6–17 was—at least in part—a substitution of children originally covered by the CHIP program.
However, since CHIP enrollment continued to grow in 2014 (Figure 2, page 2), the number of children who switched from CHIP to Medicaid was less than the total number of children who were added to CHIP during that same time period.
Conclusion
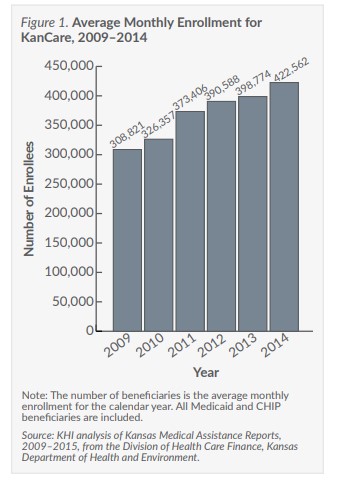
The KanCare population grew faster in 2014 than it did in 2013—with nearly all of the growth coming from children and families in Medicaid, but not CHIP. Several reasons for the growth could be attributed to policy changes occurring before the implementation of KEES, reductions in eligibility for cash assistance, and changes in Medicaid and CHIP eligibility.