



This blog series on the COVID-19 Vaccine Rollout in Kansas featured coronavirus policy tracking in 2021, with a focus on the distribution of the COVID-19 vaccines and related federal and state policy developments. More current policy tracking on the pandemic can be found in a new blog page posted March 11, 2022, at A Kansas Twist — COVID-19: Are We Out of the Woods Yet?
Sign up here to receive these summaries and more, and also follow KHI on Facebook, Twitter and LinkedIn. Previous editions of A Kansas Twist can be found on our ARCHIVE PAGE.
Vaccine Passports
By Carlie J. Houchen, M.P.H., Linda J. Sheppard, J.D., and Charles Hunt, M.P.H.,
This has been another busy month for those closely monitoring the COVID-19 vaccine rollout and related policy developments. As of May 2021, over two million doses of COVID-19 vaccine have been administered to Kansans, resulting in 46.3 percent of Kansans receiving at least one dose. Additionally, on May 10, the U.S. Food and Drug Administration updated the Emergency Use Authorization of the Pfizer/BioNTech COVID-19 vaccine to allow adolescents age 12-15 to receive it.
During the 2021 Kansas legislative session, legislators considered a number of vaccine policy issues. Senate Bill (SB) 212 would have removed the regulatory authority of the Secretary of the Kansas Department of Health and Environment to determine vaccine requirements for children in childcare facilities and for school attendance, and instead would have listed such requirements in statute. SB 213, which was considered and eventually amended into SB 212, would have prevented employers from requiring any vaccine by making it unlawful to take any adverse action against an employee because of their decision to receive or not receive a particular immunization. SB 212, as amended to include SB 213, passed out of committee but did not pass the Senate after a roll call vote in the Senate to amend it into House Bill (HB) 2224 failed. Lastly, House Concurrent Resolution (HCR) 5017 — which supported adoption of the COVID-19 Vaccine Bill of Rights related to decisions regarding taking the vaccine — was introduced, but not acted upon. Both SB 212 and HCR 5017 remain alive for further discussion next year as this was the first year in the legislative biennium.
Additionally, an item prohibiting the expenditure of state funds related to vaccine passports, defined as “written or electronic documentation of an individual’s COVID-19 vaccination status,” was included as a proviso in the budget that passed both chambers. Specifically, the budget provision says that state agencies shall not expend any money from the state general fund or from any special revenue fund during the fiscal years ending June 30, 2021, and June 30, 2020, to:
-
- Issue a COVID-19 vaccination passport to any individual without their consent;
- Require an individual to use a COVID-19 vaccination passport within this state for any purpose; or
- Deny housing or refuse access to a place accessible to the general public, or separate from others in a place accessible to the general public, including entry, education, travel and services within the state, based on such individual’s COVID-19 vaccination status.
On April 5, 2021, Governor Laura Kelly announced she had no interest in pursuing a vaccine passport in the state, and she signed the omnibus budget bill that included this provision.
This high interest in vaccine policy mirrors activity in state legislatures across the country. The National Academy for State Health Policy (NASHP) has tracked bills to ban employer COVID-19 vaccine mandates in an online dashboard. These bills approach this issue from a variety of perspectives, including a vaccine passport. In total, 85 bills have been introduced in 40 states, but only two have been signed into law (Arkansas and Montana). Of the 85 bills tracked by NASHP, 77 were sponsored by Republican lawmakers. Many of these bills included reference to or were introduced in response to guidance offered by the U.S. Equal Employment Opportunity Commission in December 2020 which said employers could require employees to get a COVID-19 vaccine, provided reasonable accommodations were available. The volume of bills introduced in state legislatures to prohibit employer vaccine mandates may indicate that COVID-19 has shifted how some legislatures consider issues governing employer relationships to their employees. Due to additional concern about COVID-19 vaccine mandates, some states (e.g., Florida, Texas) have made vaccine passports illegal by issuing executive orders.
Vaccine passports also raise international considerations as global travel has been a key source of COVID-19 transmission. In February 2021, the World Health Organization (WHO) issued an interim position paper on the issue of vaccine passports. At that time, WHO did not support requirements for proof of COVID-19 vaccination for international travel as a condition for departure or entry. WHO cited unknowns about the efficacy of the vaccine in reducing transmission and ethical considerations, including very limited availability of the COVID-19 vaccine in low- and middle-income countries, as the basis for the position? As an interim position, it is expected to be reevaluated as more information becomes available.
The Kansas budget provision, the statement by the governor and a variety of other factors makes it highly unlikely that a vaccine passport — administered by state government — would be a mechanism by which COVID-19 transmission would be curtailed in Kansas. However, some form of COVID-19 vaccine passport may be instituted by employers, businesses and other private organizations. The significant focus on vaccine policy issues during the Kansas 2021 legislative session and in state legislatures around the country suggests that vaccines are a key health policy issue. It may be reasonable to expect a high volume of vaccine-related policy issues to be addressed in state legislatures in the coming years.
What Will it Take to Achieve Herd Immunity in Kansas? (April 23, 2021)
By Carlie J. Houchen, M.P.H., Charles Hunt, M.P.H., and Wyatt J. Beckman, M.P.H., C.H.E.S.
As of March 29, 2021, the State of Kansas entered Phase 5 of COVID-19 vaccination, meaning that all Kansans, aged 16 and older, are now eligible to receive a vaccine. Though the Centers for Disease Control and Prevention (CDC) has since announced this change nationwide, Kansas was just the eighth state to make vaccines available to all. At the time of the announcement by Gov. Laura Kelly that Kansas would move to Phase 5, the availability of vaccine likely varied across counties. While some counties had been pushing for this change, others continued to limit their vaccination efforts to those eligible under earlier phases. The Kansas Vaccine Prioritization Plan, when first published, projected that vaccination would first open to all Kansans in June. Though early efforts to track the vaccine rollout in Kansas were hampered by data reporting issues, there are several, clear indicators that vaccine supply is now outpacing demand. Along with strategies and policies to promote mask use and social distancing, an accurate understanding of vaccination trends in the state — by demographic factors, geographic area and other characteristics — will be key to significantly reducing transmission of COVID-19 in our state.
Though we cannot capture vaccine demand with precision, there are several sources of information from which we can gain an approximation. First, we have the information available from the Kansas Department of Health and Environment (KDHE). Through the data dashboard at kansasvaccine.gov, KDHE reported, as of April 22, 2021, that approximately 2.3 million doses had been distributed to vaccine providers around the state. This same source also reported that the total number of doses administered in the state was approximately 1.8 million. This suggests that vaccine providers across the state may have approximately half a million doses on hand. Additionally, more than half of Kansas counties declined additional allocation of vaccine the week of April 18.
The Kansas Health Institute (KHI) utilized Household Pulse Survey data — an ongoing federal survey that provides policy makers with valuable information about the COVID-19 pandemic on an ongoing basis — to analyze COVID-19 vaccine intent among Kansans in its March 2021 edition of Pulse on Kansas. At the time of survey, which covered the period January 6-18, 2021, 53.4 percent of Kansas adults said they had already received a vaccine or would get one. An additional 24.1 percent of Kansas adults said that they would probably get a vaccine. KHI utilized data from this same survey, collected March 17-29, 2021, and found that the number of Kansans who had already received or would definitely get a COVID-19 vaccine had increased to 69.9 percent. This corresponds with decreasing uncertainty (those who said they probably would get the vaccine, they probably would not vaccine or they would get the vaccine) about the vaccine among respondents. CDC data show that only 52.6 percent of Kansas adults have received their first dose of a COVID-19 vaccine. So, there is still a gap between those who have received a COVID-19 vaccine and those who want one. Significant efforts are still needed to get shots in the arms of Kansans most interested to receive the vaccine.
Local health departments and other county government entities have been providing vaccinations and coordinating with other providers in their communities. KHI, in partnership with the Kansas Association of Counties and the Kansas Association of Local Health Departments, surveyed county officials to gain their perspective on vaccine demand. We asked if, in the week of April 4, 2021, demand for vaccine was greater than the supply, about equivalent to the supply or if demand for vaccine was less than the supply. Of note, this was just one week after all Kansans were made eligible to receive a COVID-19 vaccine. We heard from respondents from all 105 Kansas counties in the survey. In some cases, we heard from more than one representative from a county (e.g., the local health department administrator and the emergency manager).
-
- In approximately half of the counties (54 counties, 51.4 percent), respondents said that demand for vaccine was less than the current supply.
- Only one county was described as having demand for vaccine being greater than the supply.
- The remaining counties were described as having vaccine demand about equivalent to the supply (29 counties, 27.6 percent) or respondents were unsure of vaccine demand (10 counties, 9.5 percent).
- There were no notable differences in how respondents described counties of different population densities (e.g., frontier, rural, densely settled rural, semi-urban, urban).
Note: For the eleven remaining counties, there were dissonant responses — multiple respondents that disagreed. If the only dissonant response was that one was “unsure” about demand, that county was sorted into the primary category (e.g., less, equivalent, or greater demand than supply).
KDHE has also noted the need to increase vaccine demand. Identified strategies to increase vaccine demand, include enrolling and activating provider offices, assessing awareness of vaccine availability, working with community influencers and seeking non-traditional partners. Through these and other strategies is the hard and necessary work of collaborating with communities to identify and remove barriers to vaccination, and to end the COVID-19 pandemic.
These data on vaccine demand raise more questions than answers, particularly when considered from an equity lens. Who is interested to receive the vaccine that is not getting it currently? What barriers need to be removed to allow them to be vaccinated? The newly added SVI (Social Vulnerability Index) Explorer on the KDHE COVID-19 data dashboard provides the ability to answer some of these questions. This tool allows users to view vaccination rates for different racial/ethnic groups at the county level. Additionally, the tool indicates the social vulnerability of census tracts. This could support those interested to ensure an equitable distribution of COVID-19 vaccines to identify geographic areas where barriers to vaccination need to be removed.
Kansas Distribution of COVID-19 Vaccines (March 10, 2021)
By Carlie J. Houchen, M.P.H., Hina B. Shah, M.P.H., and Wyatt J. Beckman, M.P.H., C.H.E.S.
In this installment of A Kansas Twist, we will describe the Kansas plan for COVID-19 vaccinations, examine some of the differences in how counties are implementing that plan, and highlight opportunities to ensure an equitable distribution of the vaccines.
Each state is, largely, responsible for allocating vaccine supplies among providers. Additional vaccine supplies are allocated through federally administered programs such as the Federal Retail Pharmacy Program. Generally, these providers are required to vaccinate those deemed eligible in the state prioritization plan.
The Kansas Department of Health and Environment (KDHE) posted the initial COVID-19 Vaccination Plan in October 2020. This plan provided the framework for vaccine provider recruitment, storage, communication, safety monitoring and data systems. On January 7, 2021, Governor Laura Kelly announced the Kansas Vaccine Prioritization Plan, which was informed by the independent Coronavirus Vaccine Advisory Committee (COVAC). The Kansas plan outlines five phases by which the population of Kansas will be eligible to receive a COVID-19 vaccine:
-
- Phase 1 – Healthcare workers: residents or patients in long-term care (LTC), senior housing or LTC-supported independent living; workers critical to pandemic response continuity.
- Phase 2 – Persons aged 65+; congregate settings; high-contact critical workers.
- Phase 3 – Persons aged 16-64 with severe medical risks; other critical workers
- Phase 4 – Persons aged 16-64 with other medical risks.
- Phase 5 – Remainder of the population 16+ and children.*
*Note: Subject to research on vaccine risks and effectiveness for children.
Kansas is currently in Phase 2 of vaccine distribution, which is estimated to include about 1 million people, or a third of the total population of the state. Within each phase of the state plan, local health departments can make determinations as to which subgroups within the active phase should be prioritized based on the allocation of vaccine that the county receives. The state makes adjustments to the allocations received by each local health department weekly based on the number of doses allocated to the state, the total vaccine allocated over time, the total number of people in each phase and the CDC Social Vulnerability Index.
Flexibility to prioritize different groups within each phase gives local health departments both the opportunity and challenge of incorporating equity in vaccine decision-making. For example, within Phase 2, some counties may elect to vaccinate those aged 65 and older first while other counties may select a subset of high-contact critical workers to vaccinate first. Counties also may weigh the impact on other populations at risk, including those in congregate settings, which have seen large numbers of cases across the state.
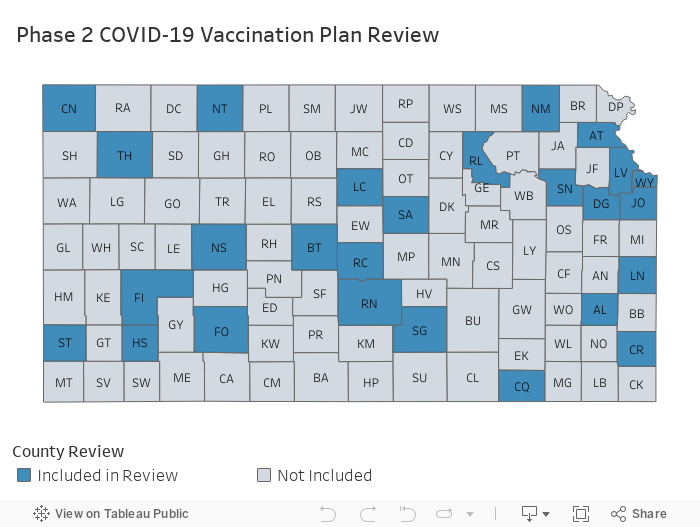
To better understand how some counties elected to vaccinate their residents, KHI reviewed vaccine plans, public announcements and social media posts for 26 of 105 Kansas counties. The 26 counties reviewed included all six urban counties and 20 additional counties from each of the four non-urban peer groups (semi-urban, densely settled rural, rural and frontier) across the six KDHE regions, covering 2,078,545 Kansans or 71.3 percent of the population (see map).
Of the 26 Kansas county plans reviewed as of March 1, only 16 counties publicly published how they were prioritizing their vaccine supply among the groups in Phase 2. By “prioritizing,” we mean the county publicly identified a specific population group as being eligible or a priority, although other population groups might not be excluded. Among the 16 counties with published details, there was much variation in how a county incorporated equity when deciding which groups to prioritize within Phase 2. Some examples include:
-
- While those age 65+ are eligible according to Phase 2 of the state plan, three (3) counties we reviewed prioritized older populations of 70+, 73+ and 85+.
- One (1) county gave a higher priority to individuals age 65 and older living in certain zip codes, using the CDC Social Vulnerability Index.
- Eight (8) counties we reviewed selected a subset of high-contact critical workers to vaccinate first (e.g., first responders, transportation workers, school teachers).
- One (1) county included low-wage, high-contact critical workers (e.g., food service workers) when identifying a subset of populations for Phase 2 prioritization.
- Two (2) counties we reviewed specifically prioritized individuals in congregate settings (e.g., behavioral health institutions, correctional facilities) when identifying a subset of populations for Phase 2 prioritization.
The remaining counties stated they were in Phase 2 and have sign up forms or wait lists that could be used to prioritize people in each phase.
To monitor vaccine distribution in Kansas, KHI also is reviewing the Kansas COVID-19 Vaccination Overview. This dashboard is regularly updated and includes a variety of key data about vaccine distribution in Kansas, such as doses distributed (1,015,940), total doses administered (658,459) and percent of Kansans vaccinated (15.1 percent) as of March 8. Additionally, the state has now published demographic information for vaccines administered. While demographic information is missing/not reported for about 15 percent of administered doses, the data available help to get a sense of who has been vaccinated to date.
The age group with the highest rate of administration is those 85+ at about 560.0 per 1,000 population. It is also notable that the rate of vaccine administration among White Kansans is about 2.3 times higher than among Black Kansans (124.1 and 54.7 per 1,000, respectively). Additionally, Kansans who are not Hispanic or Latinx have an immunization rate about 1.7 times higher than those who are Hispanic or Latinx (127.0 and 75.9 per 1,000).
If you have not yet received the COVID-19 vaccine and think you may be eligible, please utilize the VaccineFinder tool made available by the CDC.
Equity and Distribution of COVID-19 Vaccine (March 8, 2021)
By Carlie J. Houchen, M.P.H.
Scientists first published the genetic sequence for the COVID-19 virus on January 11, 2020. Fourteen months later, three vaccines have received Emergency Use Authorization (EUA) in the United States. Work is now underway to implement a critical step to protect people from COVID-19 — getting them vaccinated.
Health equity, as defined by the Robert Wood Johnson Foundation, means “that everyone has a fair and just opportunity to be as healthy as possible. This requires removing obstacles to health such as poverty, discrimination and their consequences, including powerlessness and lack of access to good jobs with fair pay, quality education and housing, safe environment and health care.” An equitable approach to vaccine distribution recognizes that vaccine supply is limited and that a variety of barriers to accessing the vaccine must be addressed. Successful, equitable vaccine distribution will require equity to be considered throughout the process.
Achieving a high COVID-19 vaccination rate will be particularly important among Black and Hispanic/Latinx Kansans, who tend to be overrepresented in jobs considered essential during the pandemic, putting them at risk of ongoing exposure to the virus. To help, the scientific and public health workforce are working to increase trust among communities of color, particularly with Black communities for whom historic failures such as the Tuskegee Syphilis Experiment, HPV vaccine development and Henrietta Lacks may be top of mind. These failures likely have contributed to lower confidence in COVID-19 vaccines in the U.S. among Black Adults, with just 41 percent indicating they had already gotten the vaccine or would get it as soon as possible, compared to 61 percent of White Adults.
The Federal Government and COVID-19 Vaccines
We start with a brief outline of the federal vaccine development process, the roles of the Food and Drug Administration (FDA) and the Centers for Disease Control and Prevention (CDC), and how it considered equity and informed the Kansas plan for vaccinations.
The FDA oversees the development and authorization of vaccines, along with the Vaccines and Related Biologic Products Advisory Committee (VRBPAC), an external advisory committee. The CDC and the Advisory Committee on Immunization Practice (ACIP) — like the VRBPAC, ACIP is a group of experts external to the Federal agencies — review clinical trial data and other research to recommend vaccination for specific populations. These independent bodies of external experts are one example of the safeguards to protect the vaccine development process from undue political, industry or other pressures. More information detailing the clinical trial process is available from the FDA online.
In June 2020, the FDA released guidance to manufacturers detailing the standards that any vaccines would have to meet before they could be authorized. The FDA provided an effectiveness threshold that would have to be met before a vaccine would be approved and strongly encouraged manufacturers to include diverse populations, specifically racial and ethnic minorities, in vaccine trials. For the Pfizer vaccine currently available, it was reported that 10 percent of trial participants were Black and 13 percent were Hispanic. Similarly, the Moderna vaccine trial included 10 percent Black participants and 20 percent Hispanic participants. Actively recruiting Black and Hispanic/Latinx clinical trial participants ensured that when the FDA was making determinations about vaccine safety, there were adequate data to state that there were no differences in safety based on ethnic or racial groups.
While the FDA and manufacturers worked to ensure that a vaccine product would be available that was safe and effective, the CDC was working on distribution plans. An early step in this process was the release of Guiding Ethical Principles by the ACIP that would inform how any recommendations for vaccination would be made. These four Guiding Principles included:
-
- Maximize benefits and minimize harms
- Mitigate health inequities
- Promote Justice
- Promote Transparency
These Guiding Principles informed how the ACIP described the phases for vaccine distribution. Subsequently Kansas, like other states, used this information to develop its Vaccine Prioritization Plan.
Since the first EUAs were issued in December, about 60 million Americans had received at least one dose of a COVID-19 vaccine by March 8, 2021. Despite this progress, concerns remain that vaccines are not always going to those who need them most. The next blog in this series will detail the Kansas plan for vaccine distribution and provide progress notes on the work in our state to vaccinate those who need it most.