FORHP Grant Programs in Kansas
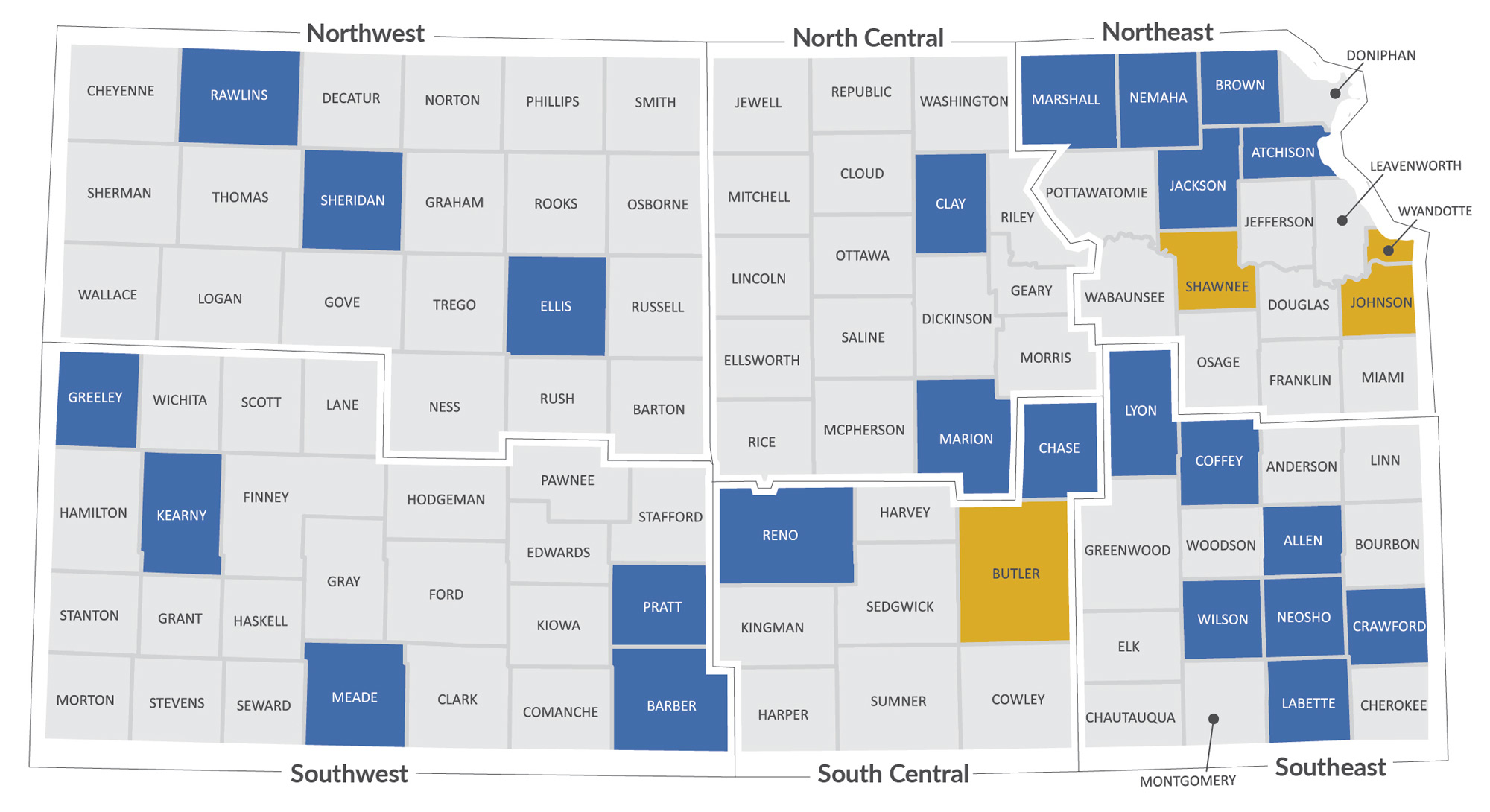
From 2019–2023, FORHP distributed 75 awards to 34 organizations in 28 Kansas counties. The organizations ranged in size, capacity and geographic location. FORHP-funded projects reached all corners of Kansas, illustrating both the wide geographic reach of these investments and their ability to address local and statewide needs (Figure 6).
One quarter of all Kansas counties saw FORHP funding awarded to a lead organization in their jurisdiction. Shawnee and Johnson counties received the most FORHP awards from 2019-2023, with 17 and 10 awards, respectively. In Shawnee county, all 17 awards were distributed to KDHE across five unique programs. In Johnson County, the 10 awards represented five different programs and were distributed to two different grantees. Those counties were followed by three rural counties — Ellis, Marshall and Sheridan — each with five awards.
The Kansas-based organizations that received FORHP funding — from large, non-rural entities to smaller, community-based groups — included the state health department, hospitals, clinics, school districts, universities, local health departments and nonprofits. This mix of local, regional, statewide and nationally focused organizations reflects FORHP’s strategy of supporting both high-capacity and community-based organizations to improve rural health.
In Northwest Kansas, Sheridan County received $800,000 (2019–2022) through the Small Health Care Provider Quality Improvement Program to improve patient outcomes. In Southwest Kansas, Greeley County Health Services, Meade Hospital District, Kiowa District Hospital and Kearney County Hospital each received between $49,000 and $150,000 from the Rural Health Clinic Vaccine Confidence Program to enhance vaccination efforts.
In North Central Kansas, Clay County Medical Center received $198,000 through the Rural Health Clinic Vaccine Confidence Program, while in South Central Kansas, the El Dorado Clinic received $50,000 under the same program. Also in South Central Kansas, Susan B. Allen Memorial Hospital in Butler County was awarded $189,000 through the Rural Health Care Services Outreach Grant Program to expand rural health care delivery.
In Northeast Kansas, Nemaha Valley Community Hospital received $300,000 through the Rural Health Network Development Program to strengthen care networks. The National Rural Health Association (NRHA), based in Johnson County, received more than $2.3 million annually (2019-2023) through the Rural Health Best Practices and Community Development Cooperative Agreement. The University of Kansas Medical Center in Johnson and Wyandotte counties received multiple telehealth focused awards, including the Telehealth Network Grant and the Telehealth Resource Center Grant.
In Southeast Kansas, Thrive Allen County was awarded $1.2 million (2019–2021) through the Rural Communities Opioid Response Program (RCORP) Planning and Implementation Program to expand substance use disorder resources.
These examples illustrate how FORHP funding supported a range of priorities during the study period — from pandemic response and behavioral health to workforce development and health care delivery — while reaching grantees across all regions of Kansas.