Understanding Disenrollment of Children From Public Health Insurance Programs in Kansas
10 Min Read
Sep 01, 2002
By
R. Andrew Allison, Ph.D.
Key Points
The Kansas Health Institute examined a new source of information made available by the Department of Social and Rehabilitation Services (SRS) to help explain why children might disenroll from the Medicaid and HealthWave programs sooner than expected. These are the primary findings:
Children whose enrollment cases are managed at a centralized clearinghouse are far less likely to be disenrolled during the first year of coverage than are children whose cases are managed at a local SRS office.
While mail-in applications to the clearinghouse have been an important new outreach tool to enroll eligible children in HealthWave and Medicaid, local SRS offices continue to enroll the vast majority of children in public health insurance.
One out of four HealthWave children who do not re-enroll at the end of their first year of coverage, when redetermination should occur, return to public health insurance within three months. The unexpectedly high number of brief lapses in coverage may be due in part to delays in completing the redetermination process.
In managing its local offices, SRS faces the dual challenge of facilitating new enrollments while minimizing premature or unintended disenrollment’s.
Background
Disruptions in insurance coverage can be costly to families and can affect children’s access to needed medical services. Previous KHI analysis of enrollment trends among children in Kansas’ HealthWave and Medicaid programs revealed high disenrollment rates during the first year of coverage. There is strong anecdotal evidence that administrative actions may be a major cause of premature disenrollment during the first year of coverage, but previous studies have not been able to quantify the potential contributions of this or any other specific factor. This study incorporates new data to identify children at risk for preventable administrative disenrollment’s.
New information
Since HealthWave’s introduction in 1999, families have been able to apply for public health insurance on behalf of their children either by mailing in a joint HealthWave/ Medicaid application to a central “clearinghouse” in Topeka or by applying in person at a local SRS office. The new data source used in this study consists of all applications mailed to the clearinghouse through June 2001. The clearinghouse is operated by Maximus, a private firm under contract with SRS, and exists for the sole purposes of assessing eligibility for, and managing enrollment in, HealthWave and Medicaid.
Families not submitting a mail-in application are presumed to have applied at a local SRS office. Unlike families that mail-in a joint HealthWave/Medicaid application, families applying at a local SRS office may arrive with the intention of enrolling in one or more of SRS’s many assistance programs, e.g., cash assistance, food stamps, childcare, health insurance. Local SRS offices were designed to administer a variety of assistance programs, providing families with a single point of contact for enrollment and case management activities, e.g., coordinating eligibility reviews and entering updated family information into the statewide enrollment database.
To facilitate the coordination of public benefits, SRS instructed local offices to manage the health insurance cases of all children whose families also participated in other programs, leaving HealthWave- or Medicaid-only cases to be managed at the clearinghouse.
Concerns have been raised that coordination of public benefits might somehow be causing premature disenrollments from public health insurance. Since our data does not identify families that participate in multiple programs, we cannot measure this effect directly. Nevertheless, we know that during the study period, there was a strong relationship between the type of health insurance application a family submitted, the likelihood that the family also was participating in other programs, and the location in which that family’s HealthWave or Medicaid case was to be managed. We take advantage of these relationships to make inferences about the effect of case management on disenrollment.
Case management
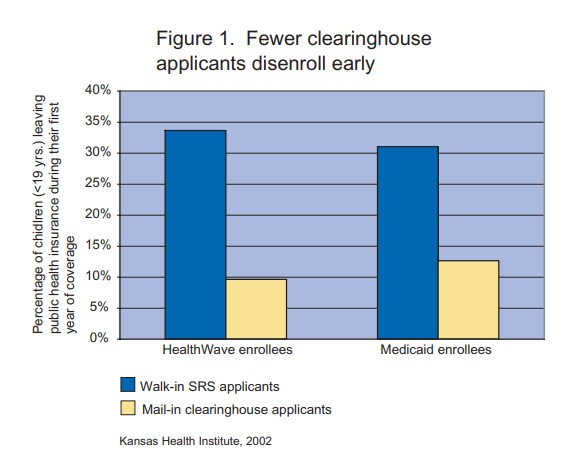
Analysis of enrollment and application records suggests that the type of application is a very good predictor of whether children will be disenrolled prematurely from HealthWave and Medicaid. In particular, the analysis indicates that first-year disenrollment rates are about three times greater for local SRS applicants than for children whose families applied to the clearinghouse. Figure 1 shows that about one-third of SRS applicants disenrolled before completing their first year of coverage, compared to about one-in-ten clearinghouse applicants.
Relying on the type of application as a proxy for the location and nature of case management, these results provide an indication of the potential contribution of case management to the overall level of premature disenrollment.
If walk-in applicants had experienced the same rate of premature disenrollment as mail-in applicants, the total number of premature disenrollees would have been reduced by over half. Of course, program administration may be only one of a number of factors that contributed to the difference in disenrollment rates between walk-in and mail-in applicants. Extensive discussions with SRS personnel, however, suggest that the high rate of premature disenrollment among walk-in applicants was indeed due to preventable administrative actions associated with the joint administration of multiple assistance programs at local offices.
An example is a local case worker setting a child’s redetermination date for public health insurance too early (i.e., before the 12 month anniversary of initial enrollment) in order to align it with the redetermination date of another SRS program that the family participated in.
Another example is a local case worker using information obtained from a family in the administration of another assistance program to review the child’s eligibility for public health insurance even before reaching the redetermination date for public health insurance. Preventable administrative actions like these may have occurred less frequently at the centralized clearinghouse, where most mail-in applicants were case-managed, because eligibility workers there did not administer other assistance programs in addition to public health insurance.
Outreach and enrollment
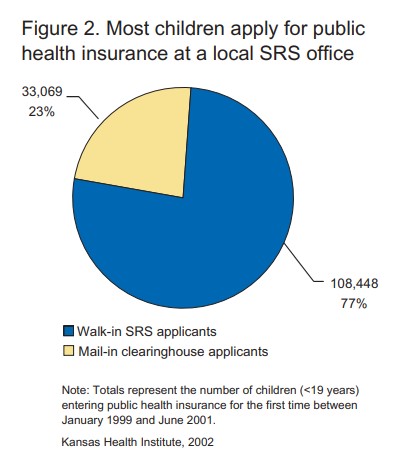
Application data used in the analysis of disenrollment patterns can also be used to estimate the number of children who have been enrolled in public health insurance as a result of the clearinghouse. SRS has reported that as many as 60,000 children were enrolled as a result of the clearinghouse between 1999 and mid-2001. However, our analysis indicates that for a comparable time period, approximately 33,000 children were 33,069 newly enrolled in 23% public health insurance as a result of having submitted a mail-in application to the clearinghouse. By contrast, nearly 110,000 children were enrolled via the traditional method of applying in-person at a local SRS office [See Figure 2]. Overall, in-person applications accounted for more than three out of four (77%) new enrollments, including over one-third (36%) of new HealthWave enrollments and more than five out of six (85%) new Medicaid enrollments.
These findings demonstrate that mail-in applications have been an important new outreach tool for children eligible for public health insurance, but that local SRS offices continue to enroll the vast majority of children. We also found a clear relationship between family income and the type of application submitted. Across the board, children in lower-income eligibility categories were much more likely to have applied in-person than children in higher-income eligibility categories, who were more likely to have applied by mail. These findings appear to reinforce the continuing importance of local SRS offices in the outreach and enrollment process.
Repeated entry and exit
“Churning” is a term used to describe the repeated entry and exit of children into and out of public health insurance. Children are considered to have “churned” if they re-enter public health insurance after a lapse in coverage. Our analysis indicates that nearly a quarter of all Medicaid children and more than one-third of HealthWave children can be expected
Insert quote on the left hand side of page 4: “Children whose enrollment cases are managed at a centralized clearinghouse are far less likely to be disenrolled during the first year of coverage than are children whose cases are managed at a local SRS office.”
to churn within 30 months of their initial enrollment. A good proportion of churning appears to occur as a result of temporary disenrollment around the time of the annual eligibility redetermination. In particular, about one in four HealthWave enrollees who leave public health insurance at the end of their first year of coverage subsequently return within three months, and another one in four return within the next 15 months.
While it is conceivable that some of the churning that occurs around the time of redetermination may be the result of families who are ineligible at redetermination but become eligible shortly thereafter, the large number of these brief disenrollment’s suggests that many families who wish to maintain coverage experience delays in completing the redetermination process.
Due in part to these findings, SRS has changed the policy for children who re-enroll after their scheduled re-enrollment date has passed. The new policy, implemented in October 2001, allows children who complete the re-enrollment process within a month following the scheduled date to be retroactively enrolled back to the scheduled date.
The role of SRS offices
The results of this study suggest that there may be potential benefits in the recent consolidation of HealthWave (Title XXI) and Medicaid (Title XIX) case management at the clearinghouse.
Consolidation was designed in part to eliminate the premature disenrollment’s sometimes experienced by families enrolled in multiple assistance programs. With consolidation, local SRS offices have retained their vital role of enrolling new participants in HealthWave and Medicaid, while case management responsibilities are now handled primarily at the clearinghouse, which appears to have the better track record for maintaining enrollment.
Unanswered questions
We have used enrollment and application data to investigate potential causes and determinants of disenrollment, but this data tracks children’s health insurance status only so long as they remain enrolled in public health insurance and thus cannot provide an answer to one of the most important questions regarding disenrollment’s: how many of the children who leave public health insurance remain uninsured?
The results presented above also lead to a number of questions about the redetermination process. How many of the disenrollment’s that occur at the time of redetermination are the result of burdensome administrative procedures? Which aspects of the redetermination process pose the greatest challenges to families attempting to re-enroll? What policy options might be available to improve re-enrollment rates? Many of these unanswered questions will be addressed in an upcoming KHI analysis of individuals who do not re-enroll at the annual redetermination.
This report was produced under contract with the Kansas Children’s Service League as part of the “Disenrollment Evaluation Project and Intervention Enhancement Training Project,” with funding provided by the Robert Wood Johnson Foundation and the Kansas Department of Social and Rehabilitation Services. The contents of this report are solely the responsibility of the author and do not necessarily represent the views of the funding organizations.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.