The supply of dentists and the way in which dental practices operate significantly affect the level of care that Kansans receive. A study of the dental workforce commissioned by the United Methodist Health Ministry Fund shows that a persistent disparity in the supply of dentists between rural and urban areas and the manner in which services are delivered are adversely affecting the oral health of rural Kansans. Further, the oral health of poor Kansans is suffering because of a lack of access to dental care. The major findings of the study are summarized below:
Key Points
-
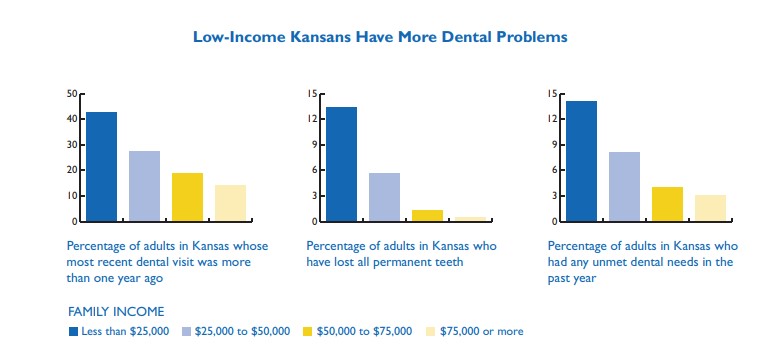
- Many poor and rural Kansans lag significantly behind an accepted standard for dental care and oral health.
- These gaps in services and care are caused in part by a limited supply of dentists—especially in rural areas.
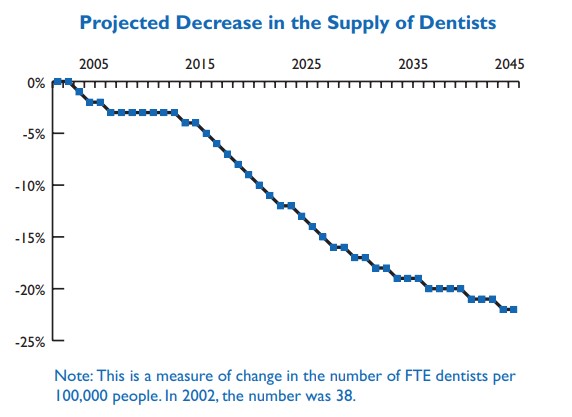
- Without policy intervention, these service gaps and resulting oral health problems will grow as the supply of dentists declines.
- State policies and workforce regulations help determine the supply of dentists and the contributions of other dental professionals to the overall supply of services.
- To improve access to dental services, policymakers could attempt to increase the supply of dentists by establishing a dental school or an in-state extension of an existing dental school, expanding education subsidy programs, or requiring more students who receive subsidies to practice in under-served areas.
- Policymakers also could target services towards underserved populations of the state, and/or support the development of new dental practice models, including expanding the types of services that hygienists or other allied professionals can provide.
- Dental workforce needs are difficult to predict and can take many years to address, suggesting the need for policymakers to monitor the dental workforce and update policies on an ongoing basis.