The COVID-19 pandemic led to rapid policy changes around telehealth in Kansas and nationwide, and policymakers are now considering which changes to make permanent.
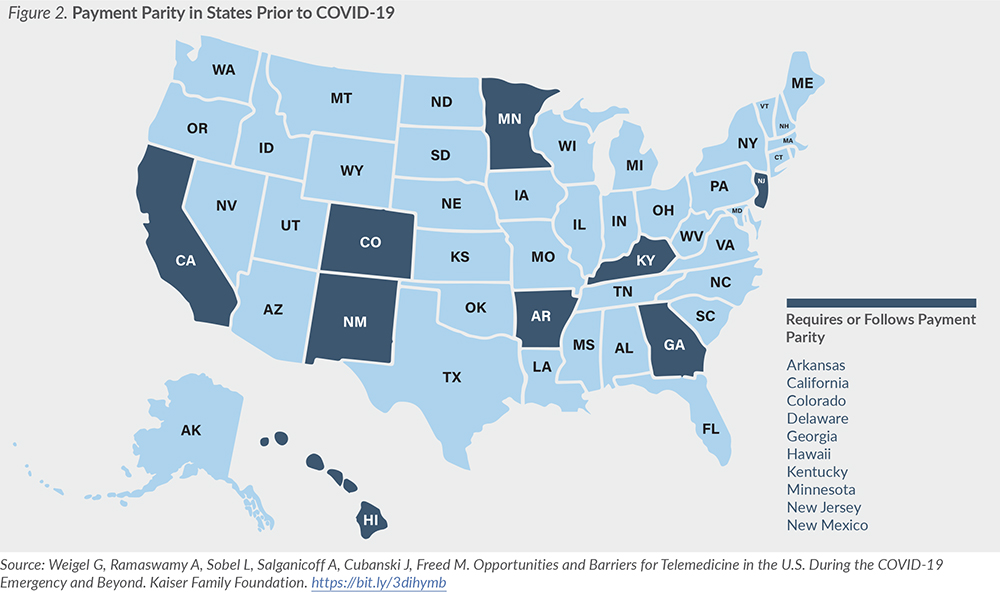
Many states have required that telehealth services be reimbursed at the same rate as in-person services during the COVID-19 pandemic, but only 10 states required this payment parity prior to the pandemic.
Patients without adequate devices or broadband may be unable to access telehealth services.
Provider interest in offering telehealth services can be hampered by high start up costs, level of reimbursement, lack of telehealth training and fears about quality of care.
This issue brief is the second of a two-part series. It explores factors that influence the utilization of telehealth and how those factors relate to the Kansas policy landscape. The first brief, Telehealth: Providing Access to Care in a Time of Social Distancing, defines telehealth, which includes telemedicine and other services, and describes its growing use and potential impact on the cost of care and health outcomes.
Introduction
Beginning in March 2020, as COVID-19 cases rose in Kansas and across the U.S., rapid changes in telehealth policy allowed providers to offer care in a socially distanced manner. Looking ahead to a post-COVID-19 world, policymakers in Kansas and around the country are now considering which policy changes should continue, which should not, and whether other changes are needed to encourage the appropriate use of telehealth moving forward.
Factors Influencing the Utilization of Telehealth
Described in more detail in the first brief in this series, telehealth can increase access to care, potentially improve health outcomes, and impact health care costs. All three factors — access, outcomes and costs — should be considered by policymakers as they debate whether and how to modify current telehealth policies.
While the use of telehealth in Medicare is largely governed by the federal government, policymakers in Kansas have multiple options to consider, from health insurance mandates to licensure laws, if they wish to expand or restrict the use of telehealth in KanCare or private state-regulated health insurance plans following the COVID-19 pandemic.
Insurance Coverage and Reimbursement
Under state laws across the U.S., health insurers can control which telehealth modalities are reimbursable, which services are covered and at what rate, and which providers are eligible for reimbursement. For example, insurers can choose to only reimburse for telehealth services provided via live video, thereby discouraging similar services from being provided via phone. This can have implications for areas with poor internet access — such as rural areas — where providing services via video may not be feasible. Alternatively, insurers can promote use of telehealth services through benefit design, such as by waiving patient cost sharing.
Telehealth Coverage in Medicaid
States are given broad authority to implement telehealth in their Medicaid programs. Prior to the pandemic, multiple telehealth services were available in KanCare, the Kansas Medicaid program, including primary care, individual psychotherapy, pharmacological management, speech-language pathology and audiology services, and home telehealth in the frail elderly (FE) waiver. However, these services could be provided only via live video and remote patient monitoring (RPM).
Like many other states, Kansas made multiple changes to the coverage of telehealth services in Medicaid following the onset of the COVID-19 pandemic. Examples of key changes include:
Requiring payment parity for telehealth services.
Expanding services allowed under telehealth, including dental services and additional services for those on home and community-based services (HCBS) waivers.
Allowing services to be provided via telephone, instead of only by live video.
Expanding allowed originating sites, including allowing a patient’s home to be an originating site, in addition to nursing facilities.
State policy documents describe the changes above as being in place until rescinded, unlike some federal changes, which are to remain in place until the expiration of the COVID-19 public health emergency declaration. While many of these policies may have been intended to be temporary, KanCare stakeholders have expressed interest in maintaining some of these changes after the pandemic subsides.
Telehealth Coverage in Private Insurance
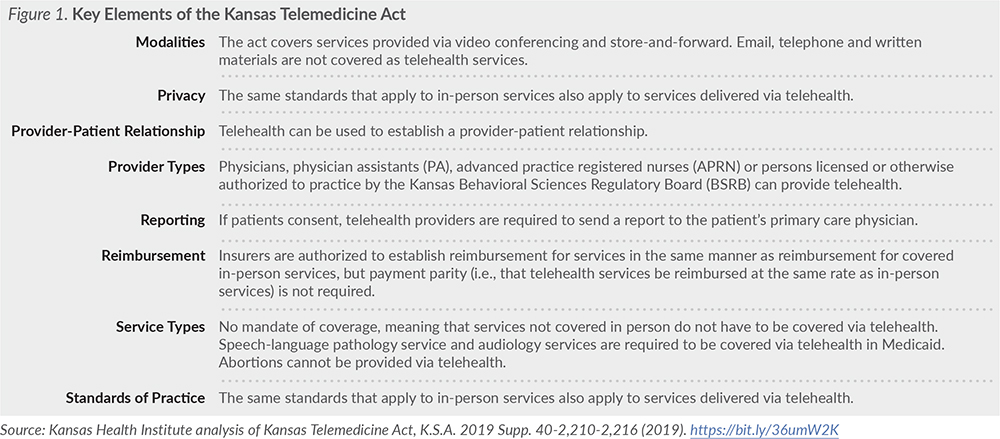
Many states, including Kansas, have laws in place governing coverage of telehealth services, but a 2017 study of state private payer laws found that the actual utilization of telehealth is impacted by how these laws are written. The Kansas Telemedicine Act was passed by the Legislature in 2018 (Figure 1).
With the onset of COVID-19, many private insurers across the U.S. took actions to encourage the use of telehealth. These actions were largely voluntary and varied by insurer. For example, some plans now include behavioral health visits as allowable telehealth visits and have increased access to these services through expanded networks. One Kansas example is Blue Cross and Blue Shield of Kansas, which expanded coverage and temporarily waived cost-sharing for all telehealth services.
In addition to actions taken by insurers, some states have enacted temporary payment parity requirements for reimbursement by private plans or have mandated that plans waive telehealth cost sharing. Prior to the pandemic, approximately 10 states required or followed payment parity for telehealth (Figure 2).
While both coverage and reimbursement of telehealth services impact how much it is utilized, other factors — such as licensure issues, provider training and broadband access — also play a large role in whether and how it is used, which can be seen in the variability of utilization across states prior to the COVID-19 pandemic.
Licensure
Typically, providers must be licensed in the state in which they are providing care to patients. Through telehealth, however, providers can offer care virtually anywhere, as long as they have an appropriate license. To allow and encourage out-of-state providers to offer telehealth, some states have joined licensure compacts or created telehealth-specific licenses. While this can increase the workforce available to treat patients, it also can lead to fragmentation of care if telehealth providers do not coordinate with a patient’s usual providers.
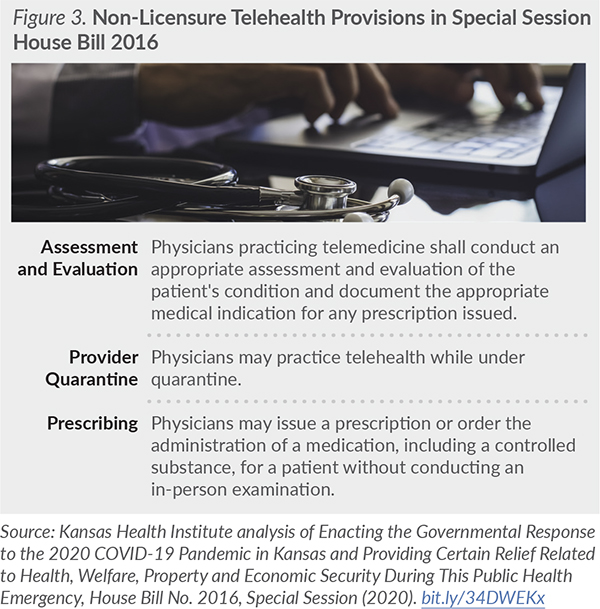
Since 2016, Kansas has participated in the Interstate Medical Licensure Compact, which allows physicians in participating states to receive expedited licensure in other states. Prior to the pandemic, the compact allowed eligible out-of-state physicians to become more quickly licensed in Kansas than the standard licensure process. Following the onset of COVID-19, Governor Kelly enacted multiple Executive Orders with provisions pertaining to telehealth, including licensure. Some of these provisions were later codified in Special Session House Bill (HB) 2016. Related to licensure, HB 2016 allows out-of-state physicians to treat patients in Kansas via telehealth without securing a Kansas license, provided certain requirements are met, such as holding an unrestricted license in another state.
The Kansas State Board of Healing Arts is authorized to extend this provision to other professions it licenses and regulates. See Figure 3 for additional components included in HB 2016 related to telehealth.
Provider and Health System Participation
Multiple barriers may prevent providers from offering telehealth services. For example, providers may lack training on telehealth, worry about the quality of care provided via telehealth or not have funds to invest in necessary infrastructure to administer it. Some providers have expressed concerns about building infrastructure during COVID-19 due to uncertainty over telehealth policies (e.g., reimbursement levels) in the future, and infrastructure costs may be particularly prohibitive to small or rural hospitals and clinics.
Health system leadership interest can likewise drive telehealth adoption across systems. Additionally, time constraints can be an issue for providers adapting to telehealth if telehealth responsibilities (e.g., responding to patients via online portals) are added onto existing patient panels. Having inadequate physical space in which to practice telehealth also can be a barrier.
Patient Acceptance and Access to Technology
Patient knowledge of and comfort with telehealth can impact its utilization. In interviews with insurers covering telehealth prior to the pandemic, they indicated that patients were reluctant to use telehealth and instead often opted for in-person services. Specific populations — like those with disabilities or older adults — may have difficulty utilizing telehealth, which requires comfort with technology and an ability to navigate the multitude of technology platforms used by providers to offer telehealth. Rapid telehealth adoption during COVID-19 may have increased some patient comfort with telehealth technology, however.
Patients also may lack access to the high-speed internet needed to receive telehealth services. This may be a particular issue for individuals in rural areas or on tribal lands, individuals of lower socioeconomic status and older adults. In addition, not all patients have access to an adequate device to receive services, such as a computer or smartphone.
Improving access to broadband has been discussed in previous legislative sessions. In the 2020 Legislative Session, for example, the legislature passed the Eisenhower Legacy Transportation program, which includes a grant program that will support the expansion of broadband services in the state.
Additionally, Kansas policymakers have allocated funds to improve the state’s connectivity infrastructure through COVID-19 funding sources, including $60 million from the federal Coronavirus Aid, Relief and Economic Security (CARES) Act. Improvements in internet connectivity could allow more Kansans to use telehealth in the future.
Conclusion
Even after the COVID-19 pandemic ends, the use of telehealth services is unlikely to return to pre-pandemic levels. Given the rapid telehealth policy changes that occurred in response to COVID-19, state policymakers will need to decide which policies to continue and which to let lapse, while also weighing the potential impacts on access, outcomes and health care costs. In Kansas, this could include considerations around which modalities and services should remain reimbursable, the rate at which telehealth should be reimbursed, and the permanent expansion of licensure options.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.