What Assumptions Changed
Federal Match Rate
Despite Democratic proposals to extend three years of 100-percent federal payment for newly eligible enrollees in states that have not yet expanded Medicaid on one hand, and the Trump pledge to repeal the ACA on the other, the law still reads that the federal government will pay a decreasing share of Medicaid expansion costs. Beginning in 2017, the federal share will decline each year until 2020, from 95 percent to 90 percent. This estimate assumes it will remain at 90 percent thereafter.
Federal match rates for those already eligible for Medicaid are modified each year to reflect changes in the states’ relative economic positions. This estimate uses the fiscal year (FY) 2018 Federal Medical Assistance Program standard match of 54.74 percent over the full seven years of the projection for that group, even though that percentage may increase or decrease from year to year.
KHI’s update also assumes the Children’s Health Insurance Program (CHIP) FY 2018 enhanced 91.32 percent match rate will revert to the lower pre-ACA level (this estimate assumes 68.32 percent) when the enhanced rate expires on September 30, 2019. If Congress were to extend the higher ACA CHIP match rate permanently, the seven-year cost of expansion to the state would be $100 million less than this estimate projects. Furthermore, the latest CHIP authorization legislation expires on September 30, 2017. However, this estimate assumes the program will not be allowed to sunset.
Population and Coverage
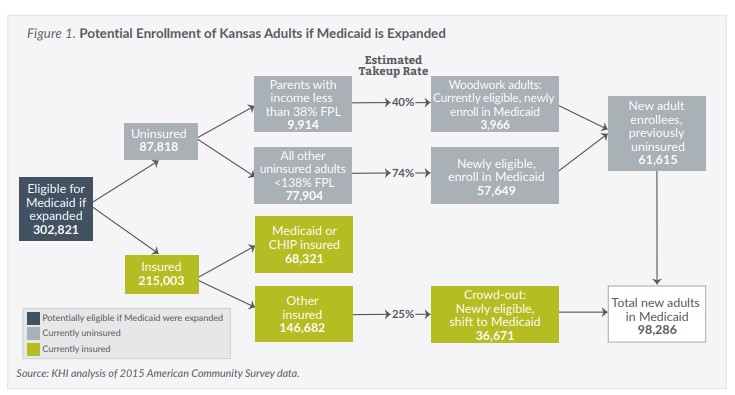
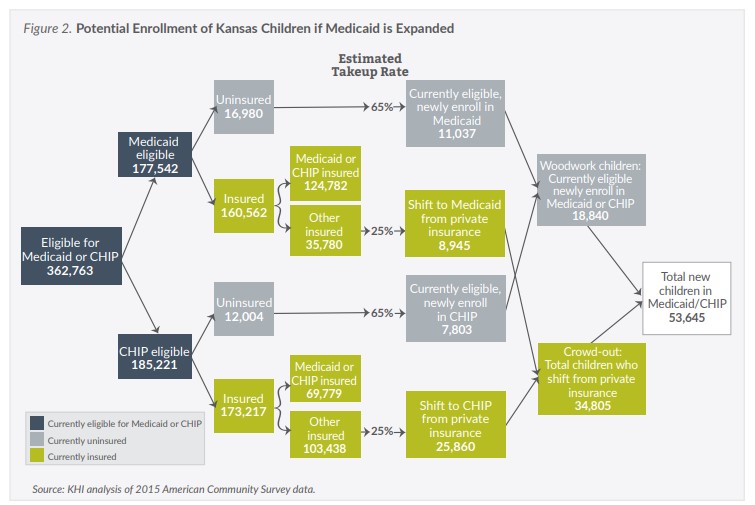
The original KHI estimate and this update use data from the U.S. Census Bureau to assess the numbers and insurance status of the population that would be eligible for Medicaid if expanded. The update uses detailed data from the 2015 American Community Survey (ACS), which reflects the second full year of implementation of the major insurance provisions of the ACA. The new ACS data show 39,000 fewer uninsured adults under 138 percent of the federal poverty level (FPL) than in the prior estimate, and 16,000 fewer uninsured children eligible for Medicaid or CHIP.
Newly Eligible Take-Up Rate
KHI’s 2012 analysis included an assumption that 65 percent of newly eligible, uninsured adults would enroll in KanCare, the state’s Medicaid managed care program. The updated estimate revises that “take-up rate” to 74 percent, consistent with assumptions in national studies.
Woodwork/Crowd-Out
The largest change from the 2012 KHI estimate to this update is related to the “woodwork” and “crowd-out” effects. The 2012 methodology included distinct take-up rate assumptions for currently eligible adults and children who at that time had not yet enrolled in Medicaid or CHIP. The assumption was that 40 percent of already-eligible uninsured adults and 65 percent of already-eligible uninsured children would enroll regardless of whether the state expanded Medicaid. This was largely because of the increased enrollment activities surrounding the ACA, and is referred to as the “woodwork effect.”
While the same take-up rates for already eligible but unenrolled members are assumed in this update, because of a decreased number of uninsured, the result is a smaller woodwork effect for both children and adults.
Estimates of the number of people enrolling because of “crowd-out,” which occurs when an already-insured, low-income Kansan switches to Medicaid, are lower than the 2012 estimate as well. In 2012, a blended crowd-out assumption was applied to all insured Kansans who would be eligible for Medicaid. In this estimate, the same 25 percent take-up rate is applied only to insured low-income Kansans who have coverage other than Medicaid or CHIP.
Enrollee Costs
The 2012 annual cost estimates per enrollee ranged from $2,351 to $4,278 for low-income adults, and $1,341 for children. Actual capitation costs for non-disabled adults age 19-64 in KanCare were $5,569 in state FY 2016. This rate approaches the 2015 national average annual per member cost of $6,366 for newly eligible adults in expansion-state managed care programs. The per member cost for non-disabled children in KanCare was $2,261 in FY 2016. The updated estimate uses the FY 2016 KanCare costs and applies a 2.5 percent annual inflation factor after 2018.
Factors Not in Estimate
Offsetting Savings
Neither the 2012 estimate nor this update assessed offsetting savings that may be achieved if Medicaid were expanded—for example, savings related to the potential elimination of optional eligibility categories or savings from state-funded programs.
Administrative Costs
Similarly, neither analysis made assumptions regarding additional administrative costs related to an expanded Medicaid program—for example, costs related to eligibility determination or program management.
Alternative Expansion Models
Some policymakers have called for the adoption of alternative expansion models that could include cost-sharing for enrollees or incorporate premium assistance for purchasing private coverage, both of which have been approved in other states. Other proposals that have not been approved yet, but may fare differently under a Trump administration, include work requirements and converting Medicaid to a block grant to the states. This estimate, however, assumes a straightforward expansion of the existing KanCare model.
What the Estimate Represents
This estimate provides an updated view of the likely effects of Medicaid expansion under current federal law by incorporating changes that have occurred over the last four years in cost, population, coverage status and enrollment.
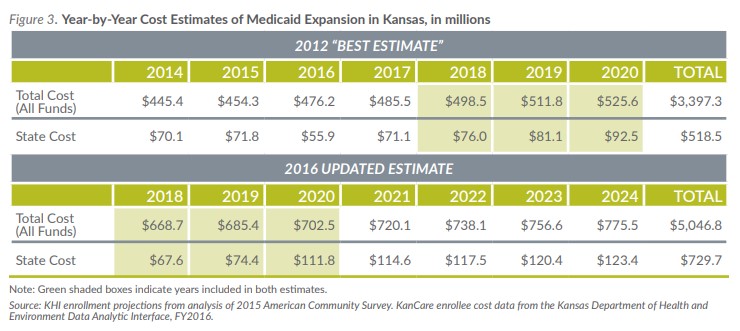
The 2012 analysis estimated a wide range of state costs, from $221 million to $912 million over seven years beginning in 2014, representing a range of take-up rates and estimated costs per enrollee. The $518.5 million “best estimate” represented a midpoint of sorts. The updated estimate of $729.7 million in state costs over seven years beginning in 2018 should also be thought of as the midpoint of another range—total state costs could be higher or lower depending on actual enrollment experience and program costs.
As the evidence from states that have already expanded Medicaid has illustrated, it is likely that if Kansas expands Medicaid under current law, enrollment and costs would vary at least somewhat from the assumptions made in this update.