


Background
Evidence continues to accumulate that the United States and Kansas are on the verge of an obesity-related health care crisis. Fully two-thirds of American adults (129.6 million persons) are overweight or obese. And despite highly visible efforts to raise awareness and help individuals make healthy decisions about nutrition and physical activity, those rates continue to increase. The health care system currently lacks capacity to respond to the projected chronic disease and disability burden that will likely result. The obesity rate in Kansas once tracked below the national average. But in recent years the Kansas rate has accelerated and now, as indicated in Table 1, may exceed the national average.
The prevalence of obesity among minorities is of particular concern. In the United States, prevalence of obesity among Hispanics and blacks is higher than among whites. Data from the National Health and Nutrition Examination Survey indicate that the prevalence of obesity among blacks in the U.S. population increased from 30.2 percent (1988–1994) to 39.9 percent (1999–2000). For the same period, prevalence among Hispanics increased from 28.4 percent to 34.4 percent. Although the percentage increase among whites was almost as high (21.2 percent to 28.7 percent), the obesity prevalence among whites remains significantly lower than among these minority groups.
It is difficult to compare minority obesity prevalence in Kansas to national estimates. The Kansas Behavioral Risk Factor Surveillance System (BRFSS) collects data annually on the prevalence of health-related conditions and behaviors, including overweight and obesity, among Kansas residents, but the prevalence of minorities in the Kansas population results in a sample size that is too small to calculate reliable estimates. Comparison of state to national estimates is desirable to establish context for the trends observed in Kansas and indicate areas of progress and/or concern. For example, the goal of Healthy People 2010, a national health promotion and disease prevention initiative, is to reduce the obesity prevalence among adults to 15 percent regardless of race and ethnicity.
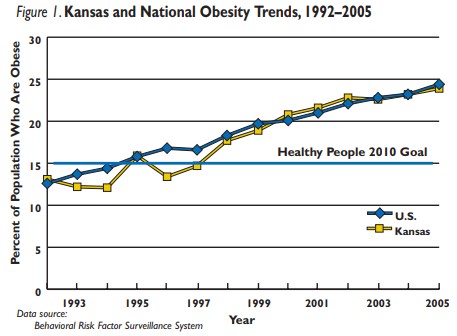
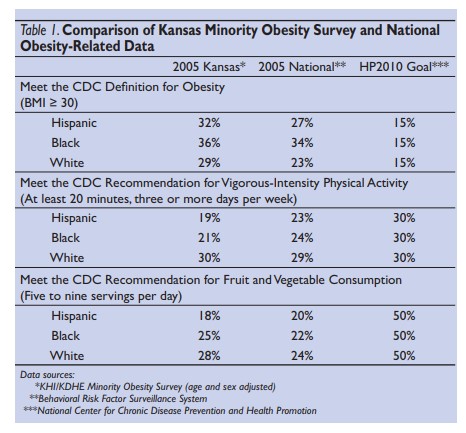
Figure 1 displays data from the annual BRFSS. It indicates that Kansas is far from the ideal obesity prevalence goal and is heading in the wrong direction. While this is an alarming observation, the situation may be even worse. As previously noted, this annual survey does not include sufficient numbers of minority respondents to permit detailed analyses of these subgroups. However, when the Kansas Health Institute, in collaboration with the Kansas Department of Health and Environment, conducted a supplemental survey that over-sampled black and Hispanic households, the survey indicated obesity prevalence among Kansas minorities exceeded the national average. It showed the same for white Kansans. Highlighted results of this survey along with comparisons to national estimates and goals are shown in Table 1.
Table 1 Highlights:
-
- For all ethnic groups, the estimate of obesity prevalence is higher in Kansas than the national average. Kansas minorities mirror the national trend in that blacks and Hispanics have higher obesity prevalence’s than whites, with blacks having the highest overall obesity prevalence. Obesity in Kansas minorities is more than twice the national goal.
- Vigorous-intensity physical activity is known to be protective against obesity. Although white Kansans are meeting the national goal for vigorous intensity physical activity and slightly exceed the estimates for other U.S. whites, black and Hispanic Kansans have lower vigorous-intensity physical activity levels than their national counterparts and are far short of the national goal. It is interesting to note that in both state and national comparisons, Kansas minority groups have noticeably lower levels of vigorous intensity physical activity than whites.
- Low consumption of fruits and vegetables is associated with higher levels of obesity. Currently no ethnic group, either in Kansas or the United States, is close to meeting the goal for the recommended number of daily fruit and vegetable servings. However, black and white Kansans are doing slightly better than their national counterparts. Hispanics, both in Kansas and across the United States, have the lowest reported consumption of fruits and vegetables and Hispanic Kansans lag considerably behind all other groups.
Key Findings
Overweight and obesity are due, in large part, to poor nutrition and lack of physical activity. Only about one in five blacks and Hispanics meet the CDC recommendation for vigorous-intensity physical activity, whereas about one in three white Kansans do. Obesity rates in Kansas are higher than the national average. In part, the relatively low levels of physical activity in Kansans can be explained by the finding that a higher percentage of adults in Kansas than nationally have jobs that promote sedentary behavior. When asked to indicate the physical activity level that best describes their work, 69 per
Poor nutrition also contributes to the high obesity prevalence in Kansas. Fewer than 30 percent of Kansans consume the daily recommended servings of dairy, fruits and vegetables. Approximately one in four blacks and whites in Kansas and fewer than one in five Hispanics meet the CDC recommendation for fruit and vegetable consumption. Twenty-seven percent of adults surveyed said that they never eat breakfast, a habit associated with poor nutritional intake. On average, adults reported that they eat out 2.8 times per week, putting their ability to make nutritious food choices, regulate portion sizes, and control food preparation at risk.
The survey also was able to identify underlying differences among the racial and ethnic groups in food purchasing considerations, providing some insight into eating behavior and diet composition (Table 2). Although approximately two-thirds of the respondents said they think that nutrition is important when buying food, only 37 percent of respondents said that they “always” or “almost always” read nutrition labels on food packages when purchasing food. Cent of respondents reported having jobs where they mostly sat or stood.
Recommendations
Obesity is a complex condition, resulting from genetic, social/ environmental, and personal health behavior interactions. At the most basic level, obesity is a problem of energy imbalance — calories consumed exceed calories that are used through metabolism and physical activities. The underlying causes of excess calorie consumption and inadequate physical activity are strongly affected by personal health behaviors interacting with genetics and the built and social environments. Detailed studies of obesity risk factors have found that personal-level factors such as consumption of processed foods high in calories and low in nutrition, limited intake of fresh fruits and vegetables, and skipping breakfast are associated with higher levels of obesity. Community-level factors also influence the risk for overweight and obesity. Availability and accessibility of grocery stores that offer healthy foods at affordable prices, public and private fitness areas and facilities, number and proximity of fast-food restaurants and convenience stores, and availability of safe walking venues each affect the choices available to individuals. Finally, the risk of obesity is influenced by sedentary behaviors such as the amount of time spent watching television and sitting at a computer, which can be associated with types of employment. Put simply, people who don’t move enough are more likely to be overweight or obese. Reversing the obesity trend will require coordinated efforts from multiple sectors (i.e., community, health care, business). The following recommendations, while based on the results of the current study and previous research, recognize the challenge of synchronizing agendas among divergent groups.

We Propose:
-
- Repeating this survey at intervals to allow Kansas to track obesity trends in minority populations. This trend analysis would provide an opportunity to measure and evaluate changes in obesity and related health behaviors and facilitate the evaluation of statewide or local interventions and efforts.
- Investigating the basis for the underlying differences in health risk behaviors of racial/ethnic minorities. Although differences were documented by this study, the reasons for them remain unknown. Given these differences, it is highly probable that intervention strategies must be culturally tailored to be effective.
- Convening stakeholders from health care, government, business and community advocacy groups (at the neighborhood level) to promote local awareness of the problem and investment in proposed solutions. Community input is essential to ensure that culturally sensitive health messages are incorporated and specific social, physical, and/or environmental influences are acknowledged.
This study confirms previous research on overweight and obesity in Kansas. It indicates that the prevalence of overweight and obesity in Kansas is high compared to national averages. Additionally, it provides conclusive evidence, similar to national reports, that the prevalence of overweight and obesity among adult Hispanics and blacks in Kansas is greater than the prevalence among whites and that the difference is driven by dissimilar health risk behaviors. Further study is required to understand the reasons for these disparities.