Introduction
The rates paid to managed care organizations1 (MCOs) and providers affect the ability of the Medicaid program to ensure beneficiaries have access to quality health care. MCOs and individual providers may choose not to participate in the Kansas Medicaid program if payment rates are set too low. The state, on the other hand, must set rates within boundaries determined by fiscal considerations and regulatory limits.
In November 2000, the Kansas Health Institute convened a group of legislators, provider representatives, state agency officials and other policymakers to discuss issues around Medicaid managed care payment rates in Kansas. As a follow-up, this issue brief will expand on that discussion. Specifically, the brief will provide background information on the Kansas Medicaid managed care program; a discussion of Kansas rates and their potential impacts; an overview of how rates are established; a summary of financial issues; and a glossary of terms.
Medicaid Managed Care in Kansas
During the 1990s, a large number of states began implementing managed care within their Medicaid programs. Reasons for implementing Medicaid managed care included the need to control costs due to overprovision of services in the fee-for-service environment and to improve beneficiary access and continuity of care.2 Joining a growing national trend, Kansas passed legislation in 1993 and 1994 requiring the Department of Social and Rehabilitation Services (SRS) to implement managed care in the Medicaid program. In Kansas, Medicaid managed care takes two different forms, capitated managed care and primary care case management. Certain Medicaid participants, largely low-income women and children, are required to participate in managed care.
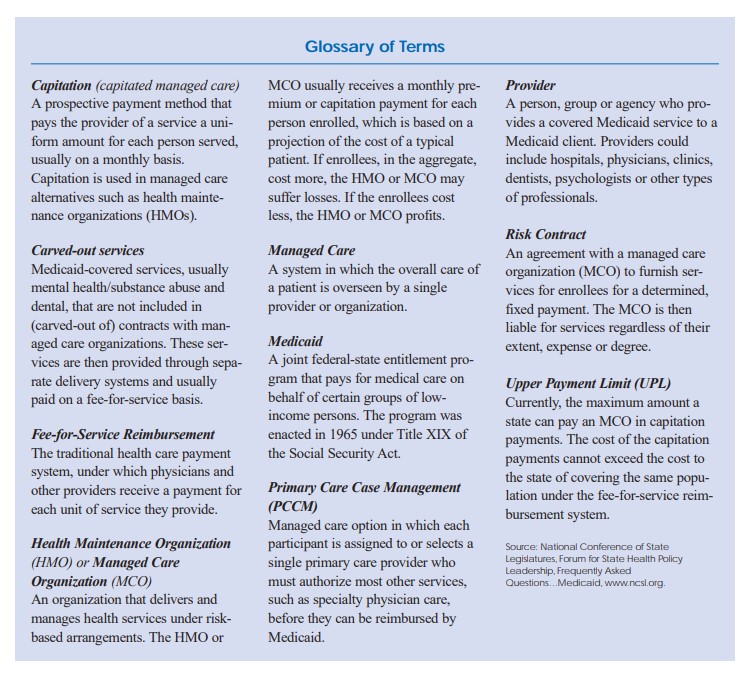
In the capitated managed care system, SRS pays an MCO a fixed sum per enrollee — a capitation rate — for a required set of services to be delivered to each Medicaid beneficiary enrolled in the MCO. This form of payment is intended to transfer to MCOs the financial risk for beneficiaries who require services that are more costly than the fixed sum they received from the state. In addition, the MCOs, and not the state, are primarily responsible for recruiting sufficient providers to maintain access for the beneficiaries. However, SRS, by federal law, still maintains ultimate responsibility for assuring beneficiaries have access to services. The MCOs negotiate a fee schedule with providers which may or may not mirror the Medicaid fee-forservice schedule. Kansas’ capitated program (formerly known as PrimeCare Kansas) has recently been blended with the State Children’s Health Insurance Program and is now part of the HealthWave program. Mental health and dental care are carved-out of the benefit package MCOs are required to provide. These services are provided through a separate system of care. Medicaid capitated managed care is available in 63 counties.
The Primary Care Case Manager (PCCM) model is a more limited form of managed care. Under this system, SRS contracts with physicians who, as PCCMs, take responsibility for coordinating beneficiaries’ care in exchange for a monthly fee of two dollars per beneficiary. Individual services provided by the PCCM or through referral are paid on a fee-for-service basis. Kansas’ PCCM program is called HealthConnect Kansas and is available statewide. This issue brief will focus only on the capitated form of managed care.
Key Questions for Policymakers
-
- Given the potential effect of low Medicaid payment rates on provider participation and beneficiary access, how can Kansas balance the desire to improve or maintain access and the need to be fiscally responsible?
- The state’s ability to increase capitation rates currently is dependent on fee-for-service rates. If federal constraints on capitation rates are reduced or eliminated in 2002, how will Kansas respond given the potential costs involved?
- In light of the challenges encountered thus far, what is the level of commitment Kansas has to Medicaid capitated managed care?
Capitation Rates and Their Potential Impacts
MCOs typically consider the capitation rates paid by SRS for Medicaid patients to be too low. Health care providers in Kansas also believe that the payment rates they accept from Medicaid MCOs are too low. Research indicates that reimbursement rates can affect both access to health care services and health outcomes for Medicaid beneficiaries.3 The adequacy of the established rates can be examined from several perspectives. These include comparisons between Kansas rates and rates paid by other states and assessments of beneficiaries’ access to health care services.
Comparisons to Other States
Assessing rate adequacy by comparing Kansas to other states is helpful, but comparison studies should be used with caution. Inter-state comparisons are complicated by many factors including variations in how states set rates, the use of different age categories, the use of rate adjustments by some states for special services and differences in the services included in the capitation rate. Also, rates considered adequate in one state may not be in another, so comparisons by themselves do not indicate the relative adequacy of a state’s reimbursement rates. With these points in mind, consider the following studies:
-
- Preliminary information obtained from the Maternal and Child Health Research Center in Washington, D.C., shows that 1999 Medicaid capitation rates for children in Kansas were the lowest of 42 states included in a comparison study.4 Kansas capitation rates ranged from 25-33 percent of the national average. Kansas rates remained low when compared to other states that also carve-out services such as mental health and dental care from the capitated benefit package. In this second comparison, Kansas rates were 40 percent of the national average.
- Another study comparing Medicaid rates across states for all low-income families and pregnant women in capitated managed care provides similar information. This study based on 1998 rates ranks Kansas near the bottom with only California, Florida, Georgia and Tennessee ranking below Kansas. Kansas rates were 82 percent of the national average.5
- A 1997 study of the Medicaid physician fee schedule found that Kansas rates were approximately 84 percent of a four-state average.6
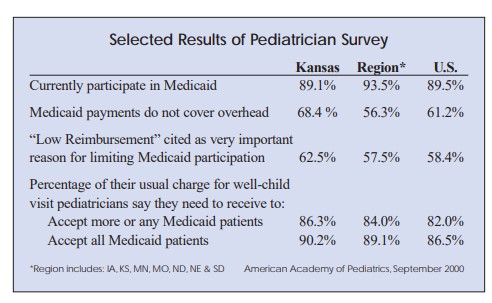
- Information from the American Academy of Pediatrics’ Medicaid Reimbursement Survey for 1998/1999 that examined selected fee-for-service rates suggested that although the selected Medicaid fee-for-service rates in Kansas compared more favorably to other states than capitation rates, they were also below the national average.7
Access to Health Care Services
Improving access to services was one of the original goals in implementing managed care and continues to be an important issue for states. The degree to which beneficiaries have adequate access to health care services can be difficult to measure. One method of measuring access is by examining the availability of health plans and providers in the Medicaid program.
The issue then becomes the causal relationship between payment rates and participation.
Health Plan Participation
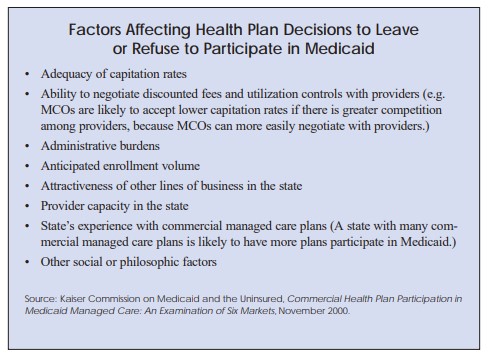
After an early influx of commercial MCOs into Medicaid in the early 1990s, a growing number of MCOs are exiting the program or are hesitant to take on Medicaid business due in part to inadequate capitation rates.8 The issue of low capitation rates in Kansas became apparent when two of the state’s three Medicaid health plans dropped out of the program at the end of 1998 largely due to low rates. The only remaining MCO, Horizon Health Plan, went out of business in the spring of 1999. Its Medicaid business was assumed by First Guard Kansas, which is now the only Medicaid health plan in the state.
In 2001, for the first time, Kansas requested bids from health plans to serve participants in both the Medicaid and State Children’s Health Insurance Program (HealthWave). The blended program began operation in October 2001 under the name HealthWave. During the bidding process, it became more clear that low Medicaid capitation rates affect the state’s ability to contract with MCOs. Only one health plan, First Guard Kansas, bid on the blended program and was awarded the contract. According to information from SRS, a second MCO that had been involved with HealthWave since its implementation declined to bid on the blended program citing low Medicaid reimbursement rates as a financial risk it was unwilling to accept.
A number of hypotheses have been put forward to help explain why MCOs are making the decision to exit or refuse to enter Medicaid. Some of the factors cited are listed in the box on this page.9 Another factor may be the level of provider capacity in the state. Proposed federal regulations to implement portions of the Balanced Budget Act of 1997 may also negatively affect the willingness of MCOs to participate in Medicaid in the future, because the regulations would impose significant administrative responsibilities on states and MCOs.
Provider Participation
Research indicates that provider decisions on whether to participate in Medicaid or the number of Medicaid clients existing providers are willing to see are affected by payment levels.10 However, as with health plans, reasons for participation or non-participation in Medicaid are more complex than payment amounts alone. The bigger question is whether participation rates are adequate to serve Medicaid beneficiaries. This question can be difficult to answer because it is not only the number of providers but also the number of beneficiaries they are willing to see and the amount of capacity open in their practices that determine adequacy.