Disabled Population
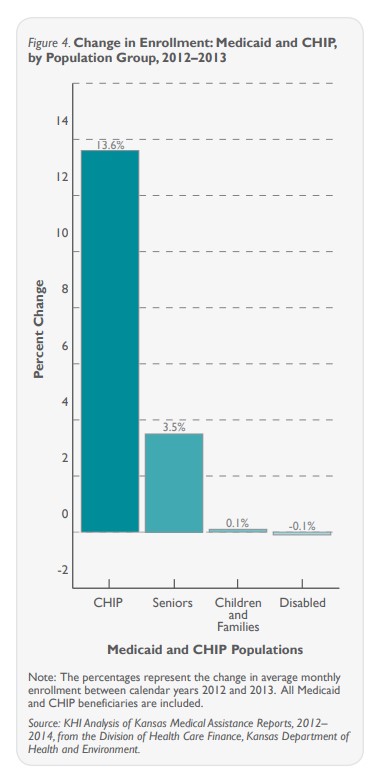
Enrollment was also essentially flat (-0.1 percent) for individuals with disabilities during the first year of KanCare. While individuals with disabilities received health care services through KanCare in 2013, home and community services for people with developmental disabilities were “carved out” until January 1, 2014.
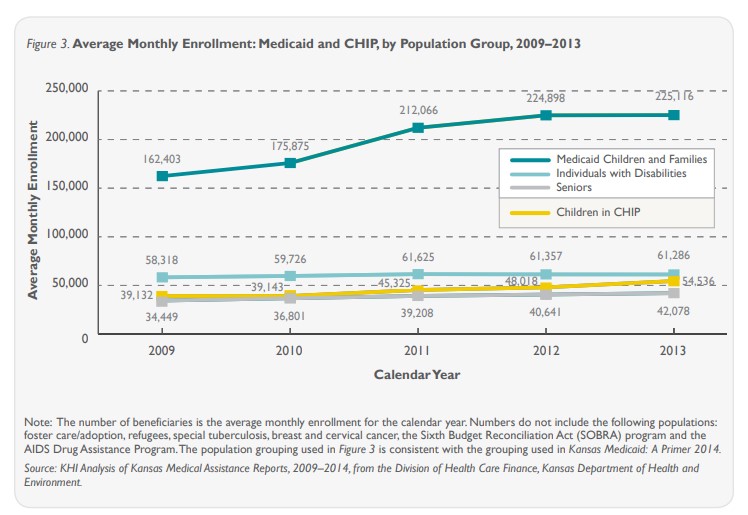
Annual enrollment growth for individuals with disabilities ranged from -0.4 to 3.2 percent between 2009 and 2012.
Seniors
Low-income individuals age 65 or older are eligible for coverage under both Medicaid and Medicare (a federal health insurance program for this age group). This population grew 3.5 percent between 2012 and 2013 —slightly lower than historical growth trends which ranged from 3.7 to 6.8 percent between 2009 and 2012.
Impact of Economy and Policy
The shift to KanCare did not change eligibility rules for Medicaid or CHIP. Therefore, the new program is not likely the cause of the lower enrollment growth in Medicaid, nor for the significant increase in CHIP enrollment. Economic conditions and policy changes are two factors more likely to have affected how many people enrolled in Medicaid and CHIP during this time.
The Kansas economy has continued to improve since the 2008 recession. Unemployment rates declined between December 2012 and December 2013 (6.5 percent to 5.7 percent) and personal income levels in Kansas increased by 2.3 percent in 2013. These economic trends generally result in slower enrollment growth, as fewer people are eligible for programs like Medicaid and CHIP.
Enrollment also was affected when Kansas Medicaid underwent several significant policy changes.
Elements of the Affordable Care Act (ACA) began impacting Medicaid in late 2013. The federal government increased awareness of health insurance options and created mechanisms to reach out to Kansans about available options through the ACA. In October, open enrollment began through the health insurance marketplaces created by the ACA. As part of the enrollment process, the marketplaces screen applicants for eligibility for tax credits to help them purchase health insurance and also for eligibility for Medicaid or CHIP.
While the rollout of the online marketplaces was riddled with technical problems, the Centers for Medicare and Medicaid Services report the marketplaces identified 5,508 Kansans who were eligible for Medicaid or CHIP through December 2013. Therefore, the marketplace rollout likely should have increased enrollment in KanCare.
The ACA further impacted Medicaid enrollment by requiring states to align their Medicaid and CHIP application process with the marketplaces’ process, as a “no wrong door” approach for low-income families.
The state implemented an online application portal in 2012 as an alternative to paper processing, which may have made it easier for some families to apply. All of these efforts would be expected to increase enrollment in KanCare.
Although Medicaid’s online application tool may have been helpful to some applicants, there may have been added confusion with the troubled rollout of the ACA’s marketplace website. All of these issues, along with other state policy or administrative factors, may have affected KanCare enrollment.
Conclusions
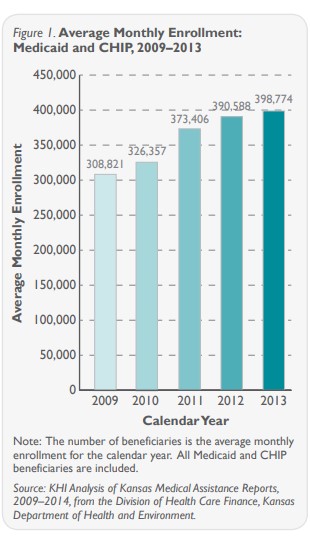
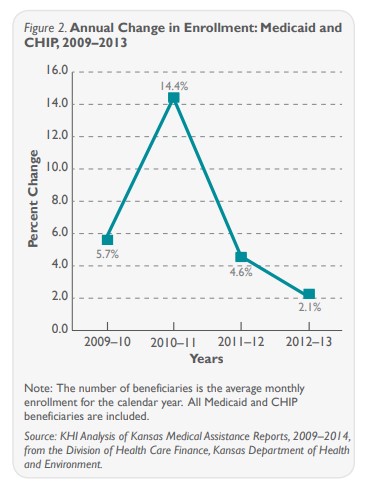
The rate of growth in the Medicaid and CHIP population during the first year of KanCare was 2.1 percent. This is a historically low rate of growth compared to the previous four years in Kansas.
An improved economy, along with increased awareness of insurance options due to the ACA, may be contributing factors. Because the shift to KanCare did not change eligibility rules or the application process, it is unlikely the program influenced the lower growth rates.
It will be important to continue monitoring enrollment, particularly for children and families in Medicaid. Most researchers expect to see increased enrollment for these populations in 2014 as the ACA heightens awareness of the Medicaid and CHIP programs.