Background
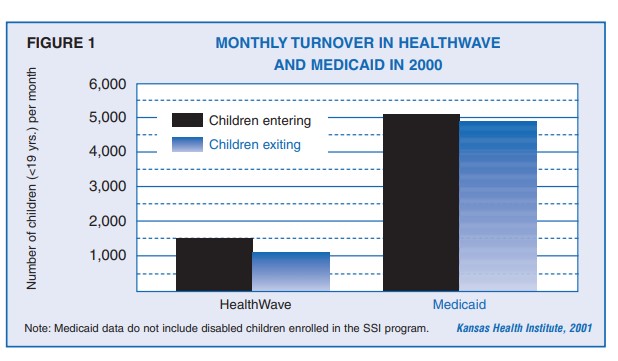
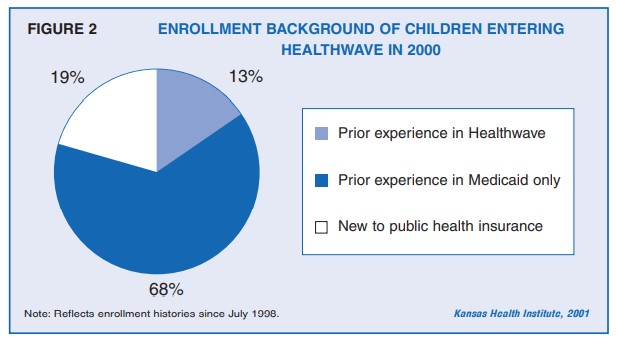
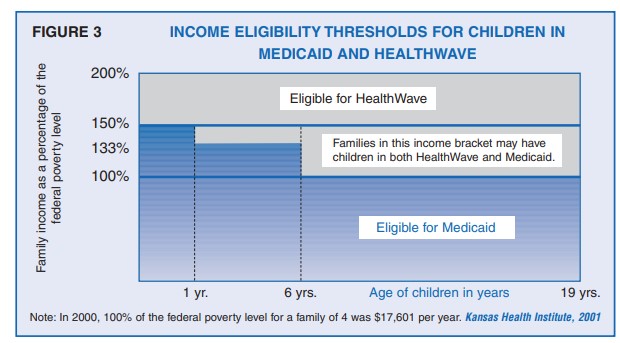
The recent growth in the number of children enrolled in HealthWave and Medicaid is well-documented. This Issue Brief examines the dynamics underlying this growth, focusing on the movement of children into, out of, and between the two Kansas programs that provide health insurance to eligible low-income children.
Data
Data obtained from the Kansas Department of Social and Rehabilitation Services (SRS) consist of enrollment records for non-disabled children under 19 years of age who were enrolled in the Medicaid or HealthWave programs between July 1, 1998 and June 30, 2000.
Kansas HealthWave Evaluation Project
This three-year, $1.4 million evaluation of the new HealthWave program includes a survey of 1,500 HealthWave and Medicaid families, focus groups with HealthWave families, analysis of enrollment and other administrative data, and extensive discussions with program administrators and health care providers from around the state. The project runs through September 2002. KHI serves as the lead organization for the project, where Robert St. Peter, M.D., is the principal investigator and R. Andrew Allison, Ph.D., is the project manager and co-investigator.
Collaborating Organizations
-
- Kansas Health Institute
- Kansas Department of Social and Rehabilitation Services
- Kansas Department of Health and Environment
- University of Kansas: School of Social Welfare
- University of Kansas Medical Center
- Department of Health Policy and Management; School of Nursing
- Department of Preventive Medicine,
- School of Medicine-Wichita Kansas State University: Survey Research Laboratory
- Kansas Foundation for Medical Care
Organizations Funding the Project
-
- U.S. Agency for Healthcare Research and Quality
- David and Lucile Packard Foundation
- Kansas Health Foundation
- United Methodist Health Ministry Fund
- Prime Health Foundation