Introduction
Public health funding in Kansas and the nation has decreased in recent years, while the responsibilities of public health agencies have remained the same or increased. As resources become more limited, public health departments throughout Kansas are being forced to explore alternate ways to effectively and efficiently provide foundational public health services in their communities.
Cross-jurisdictional sharing (CJS) arrangements among counties provide one potential solution to this challenge. CJS is the deliberate exercise of public authority to enable collaboration among two or more jurisdictions, like counties. CJS can increase effectiveness and efficiency by allowing public health officials and policymakers to pool resources with other jurisdictions in order to make a larger impact on health.
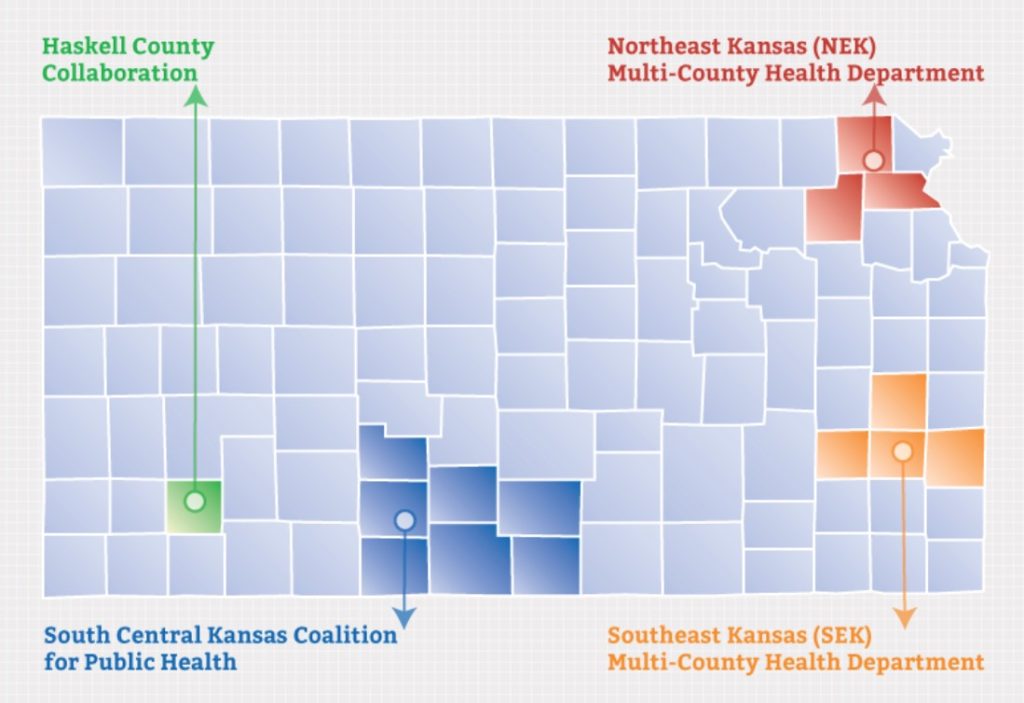
The Kansas Health Institute (KHI) recently developed case studies that explore the perceived benefits and challenges of four existing public health CJS arrangements in Kansas. Those collaborations are the Northeast Kansas Multi-County Health Department, South Central Kansas Coalition for Public Health, Southeast Kansas Multi -County Health Department and a public health collaboration between Haskell County and the Satanta District Hospital (see insert). All of the arrangements are located in rural settings. Three of the four collaborations each serve combined populations of around 35,000-40,000. The other is a public-private partnership that involves a single county and serves a much smaller population. All of the sharing arrangements have been in place for more than 20 years.
Information for the case studies came from interviews conducted by KHI between March and July of this year with key public health personnel involved in the collaborations. The individual case studies can be found online at www.khi.org/policy/article/kansas_cjs. This issue brief was developed to share information about common themes, benefits and challenges of these CJS arrangements with health department administrators, local policymakers and other interested stakeholders.
Common Themes
While unique benefits and challenges were identified within each CJS arrangement, several common themes emerged from the case studies.
Limited Resources
Each arrangement began when community members, policymakers and/or public health administrators saw a need to efficiently provide public health services in small counties. Because these areas had limited resources to fund public health activities, leaders considered pooling resources and populations with other counties in order to build economies of scale or meet minimum program requirements. As a result, they started conversations among contiguous jurisdictions and with community stakeholders that explored the possibility of sharing public health programs and resources in order to better serve their communities.
Many of the collaborations have shared family planning services, chronic disease risk reduction, and the Women, Infants, and Children (WIC) program. WIC was often among the shared programs because state and federal grants required a minimum population to participate in the program. Therefore, counties needed to combine their population numbers in order to qualify for the grants.
In addition, all of the collaborations share sta. in some manner—administrators, project managers, dieticians, health educators and others—between the health departments or health care providers in the partnership. This has allowed them to increase service capabilities and improve collaboration.
Governance and Funding
The sharing arrangements featured in the case studies have their own unique structures for administration and management of public health activities. The formality of the arrangements vary on the cross-jurisdictional sharing spectrum (see insert) from service-related arrangements to regionalization.
Each sharing arrangement is governed by a board of health, board of directors or an executive board. The board is either made up entirely of county commissioners or a combination of county commissioners, medical professionals and community members. In all of the arrangements, the board is responsible for approving budgets and programs, as well as providing feedback to the administrative staff.
In terms of money, each of the arrangements also has its own unique structure for ensuring funding equity between the counties and organizations involved. Each must make sure that funding is distributed fairly among the partners, either at equal portions or based on population size.
Policymaker Engagement
Gaining and keeping political support from county commissioners is important in CJS arrangements. In these four initiatives, approval from the county commission was needed in order to start conversations about developing sharing arrangements between jurisdictions. At first many commissioners were concerned about losing their county identity and autonomy. The health department administrators worked to inform their commissioners of the importance of public health and the need to provide essential public health services in their communities in an efficient and effective way. Focusing on efficiencies that would result from sharing arrangements was one way public health offficials gained buy-in from policymakers. As arrangements developed and grew, so did support from most county commissioners because they could see the sharing arrangements provided a way to deliver quality public health services efficiently.
In addition to involving county commissioners, most of these arrangements were developed with help from the Kansas Department of Health and Environment (KDHE). Various KDHE employees—such as the secretary of health, legal counsel and regional nurses— helped establish these CJS arrangements.
Evolving and Transforming
Throughout the years, the partnerships have gone through several transformations. Some CJS arrangements lost partner counties due to financial and political pressures. Many CJS arrangements made shifts in personnel and operations in order to accommodate new shared services. As counties saw the need for certain positions—such as health educators or project managers—they created those positions and evaluated their effectiveness. Over time, it became apparent that some positions were not as efficient as planned; for example, sometimes too much driving time was involved. In those cases, the counties in the arrangement reconfigured responsibilities to be more effective and efficient.
Benefits
All of these CJS arrangements have resulted in an increase in quality public health programs that are delivered more efficiently than they would have been if offered individually by each county.
The number of public health programs provided in these communities has increased through the development and growth of these CJS arrangements. Collectively, these sites have added WIC, family planning, child health, immunizations, women’s health and other services.
The CJS arrangements allow counties to offer programs or services more efficiently than they could have offered them on their own. For example, counties save money by sharing staff. At the Southeast Kansas Multi-County Health Department, four counties share a public health administrator, an accountant and a medical director, which helps to reduce administrative overhead. At the Haskell County collaboration, nurses can work at both the health department and a clinic run by the hospital, which minimizes unbilled hours. In all collaborations, training costs can be reduced because only one sta. member from each collaboration must be sent to training instead of one sta. member from each county. The newly trained person can then teach important skills to others in the partnership, thus reducing registration and travel costs and better utilizing resources.
The cost to administer programs also can be reduced. For example, in the seven-county South Central Kansas Coalition for Public Health, Barber County manages emergency preparedness for the coalition, Kiowa County manages WIC and Kingman County manages family planning. This saves administration time because only one county must coordinate grant applications and reporting for each program, but the residents of all seven counties benefit from the program.
An additional benefit in all of these arrangements is that they have fostered a spirit of teamwork among the partners involved. Supportive, trusting and self-motivated teams have made these sharing arrangements successful in protecting and promoting health in the counties.
Challenges
The case studies also identified challenges to participating in public health CJS arrangements.
Because the communities studied are located in rural settings, driving time was often a substantial barrier. If shared staff members are required to drive across several counties on a regular basis, those sta. members will be less efficient because they will spend a lot of time in a car and the public health agency could be paying too much in travel expenses.
Communication between counties also was cited as a challenge. Communication works well among employees in each individual county, but constant communication with other counties in a collaborative arrangement can be difficult and requires additional effort to ensure that critical items are clearly communicated to all staff.
Measuring and evaluating the success of the CJS arrangement also was challenging. Most partners have a quality assurance or quality improvement process in place to locate gaps and areas of improvement within programs. Many of the agencies conduct regular evaluations on the delivery of shared services, often through community or client surveys. However, these types of evaluations typically are motivated by individual program requirements and do not look specifically at the benefits of sharing services. There are resource barriers—chiefly time, technical skills and funding—to conducti ng evaluations of the sharing arrangements themselves because these types of evaluations are challenging and resource intensive.
Recommendations
CJS arrangements can continue to improve by offering new services, billing private insurance or improving overall operations for the bene.t of the public’s health. Conducting regular evaluations of the CJS arrangements could reveal opportunities for these arrangements to increase their efficiency and effectiveness in the community and show value for more widespread adoption.
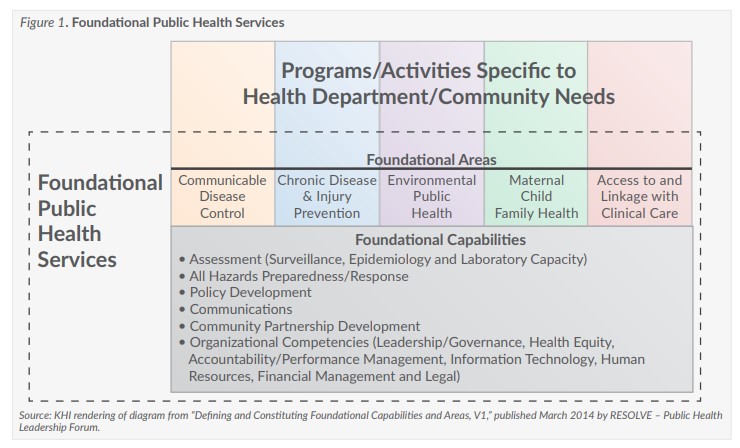
While the case studies included sharing arrangements centered primarily on clinical health services, CJS also can be used in other public health areas. For example, CJS arrangements can help counties deliver population health services or can ensure that public health departments provide the foundational public health services, which are shown in Figure 1.