In 2017, 5,405 individuals age 0-21 in KanCare had an ASD diagnosis, and 153 received ABA. While not all individuals with an ASD diagnosis likely required ABA due to medical necessity, the number receiving ABA remains low.
Most respondents to the ABA provider survey indicated that they have a waitlist, with average wait times close to two years (22.3 months) in KanCare and over a year and a half (19.4 months) for private insurance.
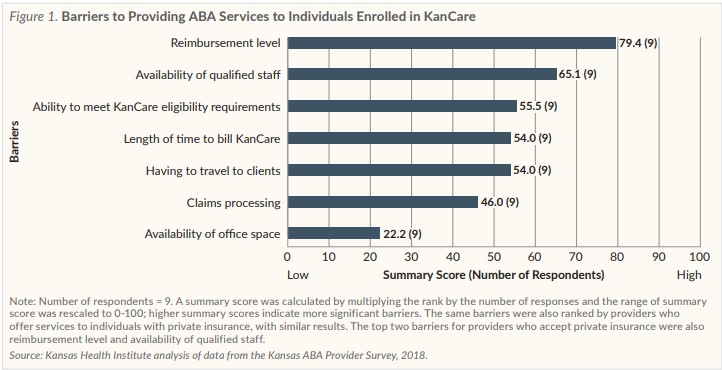
Respondents to the ABA provider survey who accept KanCare and/or private insurance indicated that reimbursement levels and a lack of qualified staff were the most prominent barriers to providing ABA services.
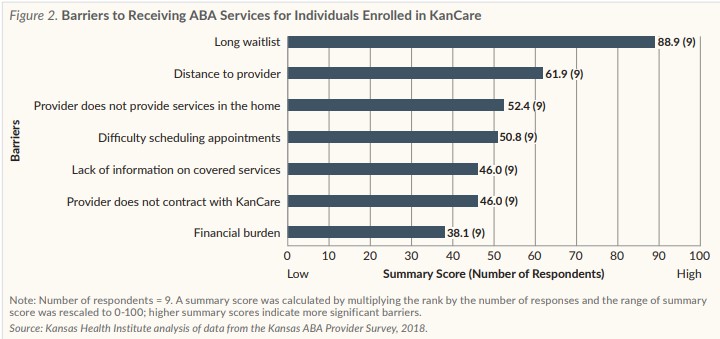
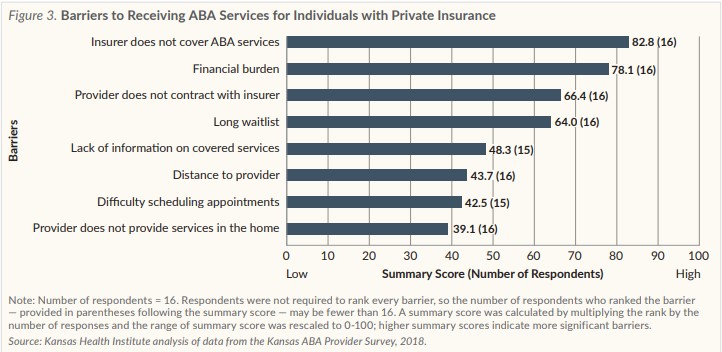
Respondents to the ABA provider survey indicated that waitlists and distance to providers were the most significant barriers families with KanCare face, while lack of coverage for ABA services and financial burden were the most significant barriers for families with private insurance.
Introduction
As the prevalence of autism spectrum disorder (ASD) has increased — up from 1 in 150 children in 2000 to 1 in 59 in 2014 — so has a national push for coverage of ASD services, including applied behavior analysis (ABA). ABA is an intensive treatment that utilizes principles of behavior and learning to modify socially significant behaviors (e.g., using positive reinforcement to encourage a desired behavior). It is typically provided in one-on-one sessions, using treatment programs ranging from 10 to 40 hours per week.
ABA is provided via a tiered service-delivery model, with behavior analysts creating and monitoring treatment plans carried out by technicians. While there are limitations with the current evidence assessing ABA, to date it appears to be the most effective treatment mechanism for ASD. In particular, ABA benefits preschool age children, and early intervention might reduce long-term costs associated with ASD.
The costs of providing ABA are high ($40,000 to $60,000 per year), however, and across the U.S. states struggle to provide ABA to individuals who need it. The cost of providing ABA, few ABA providers and long waitlists all have been cited as reasons for the lack of access. The same issues appear to be present in Kansas, even in the wake of legislative and administrative changes intended to improve coverage for ABA.
Legislative and Administrative Changes
Two major changes have occurred in Kansas in the last five years to increase coverage for ABA. In 2014, the Legislature passed a mandate requiring large group and some individual and small group health plans to cover ASD services for beneficiaries younger than 12 years of age, including ABA when medically necessary. The mandate does not apply to insurance offered by employers who “self-insure,” or essentially any individual and small group plans. In 2017, the Kansas Department of Health and Environment (KDHE) added ASD services to the Early and Periodic Screening, Diagnostic and Treatment (EPSDT) section of the state plan for KanCare, the comprehensive managed care program that combines Medicaid and the Children’s Health Insurance Program (CHIP). ASD services added to the KanCare state plan included consultative clinical and therapeutic services (CCTS) and intensive individual support (IIS) services.
ABA in KanCare
CCTS and IIS services previously had been available under the Autism Waiver, which is restricted to fewer than 100 children per year. Moving CCTS and IIS services to the KanCare state plan was intended to increase the number of individuals with ASD who could access these services. While CCTS and IIS services are referred to as “ASD services” by the state, these services are billed using Current Procedural Terminology (CPT) codes developed to report ABA services.
In 2017, 5,405 individuals age 0-21 had a diagnosis of ASD in the KanCare program, and 153 received CCTS and IIS services. While not all individuals with an ASD diagnosis likely required ABA due to medical necessity, the number of individuals receiving CCTS and IIS services in KanCare remains low relative to the number with an ASD diagnosis.
ABA Providers
One reason for the low number of individuals in KanCare receiving CCTS and IIS services (i.e., ABA) may be due to few ABA providers across the state. In December 2018, there were only 174 licensed behavior analysts (LBAs) in Kansas to serve individuals needing ABA with private insurance and KanCare, in addition to those who self-pay. In addition to LBAs, KanCare allows providers who meet state requirements (often referred to as “autism specialists”) to offer CCTS services. Data are not available on the exact number of potential autism specialists in the state. The number of CCTS providers providing services through the KanCare program is known, however. As of December 2018, there were 111 providers that include LBAs and autism specialists. Due to the intensity of ABA services, any increase in the number of individuals accessing services will require an increase in the ABA workforce.
Barriers to Providing and Receiving ABA
Information collected from a survey of consultant-level ABA providers (i.e., LBAs and autism specialists) in the state offered additional insight to potential barriers to providing ABA in Kansas. The survey was disseminated through three organizations with overlapping membership, and some providers who received the survey might not currently offer services or might offer services in settings not covered by insurance (e.g., schools). The approximate number of potential respondents ranged from 174 (the current number of LBAs in the state) to 250 (the largest membership of the three organizations who distributed the survey). The number of survey respondents retained for analysis was 34 ABA providers, providing a response rate ranging from 13.6 percent to 19.5 percent.
When asked which forms of payment they accept, survey respondents said they were most likely to accept private insurance (61.8 percent, 21 out of 34), and least likely to accept KanCare (35.3 percent, 12 out of 34). Respondents who did not accept KanCare noted the reimbursement level as the leading reason.
Access concerns appear to be present for both KanCare and private insurance, however. Of the 11 survey respondents who did accept KanCare, all indicated that they have a waitlist for children with ASD enrolled in KanCare to begin receiving services. Eleven out of 17 survey respondents who accept private insurance also indicated that they have a waitlist for individuals with ASD with private insurance. Once on the waitlist, the average time to begin receiving services for individuals enrolled in KanCare was close to two years (22.3 months), and the average wait time for individuals with private insurance was over a year and a half (19.4 months).
Among the most prominent barriers for survey respondents to offer ABA services in KanCare and private insurance were reimbursement levels and the availability of qualified staff (Figure 1). The availability of qualified staff in KanCare might be, in part, related to concerns about current training requirements for CCTS and IIS providers. While half of respondents (54.5 percent, 6 out of 11) who accept KanCare indicated that current training requirements for CCTS and IIS providers are appropriate, one-third of respondents (36.4 percent, 4 out of 11) indicated that CCTS requirements were too lax and IIS requirements were too stringent. This might stem from differences in state requirements for CCTS and IIS providers relative to requirements established by a national professional organization.
Survey respondents indicated that waitlists and distance to providers were the most significant barriers that families enrolled in KanCare face when trying to obtain services, reflecting the shortage of providers in the state (Figure 2). However, private insurance providers indicated that a lack of coverage for ABA services and the financial burden were the most significant barriers that families with private insurance face (Figure 3). Even though recent legislation mandated coverage of ABA services when medically necessary, it does not apply to all private insurance. The mandate excludes plans offered by employers who self-insure and individual and small group plans. Additionally, some families might not have updated and comprehensive information on coverage and eligibility requirements, and they might face high out-of-pocket expenses (e.g., deductibles and co-payments). This issue deserves additional analysis to better understand how well the legislative mandate has achieved its intended objective.
Limitations
Limitations should be noted for these findings. First, ASD diagnosis and medical necessity criteria determine the need for CCTS and IIS services, and this analysis lacked information on medical necessity. Second, complete information on the number of providers in Kansas is not available. Third, survey findings might not generalize to all ABA providers due to the small number of respondents. They do, however, identify issues for further exploration.
Conclusions
The state expanded training options for autism specialists in 2017, which might increase the number of providers in KanCare in future years. However, encouraging more individuals to complete trainings might be a challenge due to a disruption of state funding for provider trainings, low reimbursement rates for KanCare and private insurance and a lack of coverage by some private insurance plans.
While increasing reimbursement rates would increase health care expenditures, potential offsets could be seen through savings in other service areas (e.g., living expenses, education and supported work). The state has made changes to increase the number of individuals eligible for ASD services in Kansas; however, additional changes might be needed if policymakers would like to further increase the number of individuals actually accessing ABA.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.