



Every few years, a proposal to turn the Medicaid program into a block grant to states emerges in a new form. The concept goes back to the Reagan Administration, and more recently was part of abandoned plans in Congress to repeal and replace the Affordable Care Act (ACA). This time around, it’s more than a proposal — it’s a 56-page set of guidelines released by the Centers for Medicare and Medicaid Services (CMS) on January 30, 2020, and the topic of KHI’s latest A Kansas Twist.
Sign up here to receive these summaries and more, and also follow KHI on Facebook, Twitter and LinkedIn. Previous editions of A Kansas Twist can be found on our ARCHIVE PAGE.
The optional demonstration model outlined by CMS, dubbed the Healthy Adult Opportunity (HAO), would allow states to modify the usual rules of the joint federal-state program in exchange for cost controls in the form of block grants — called aggregate caps — or per-capita caps, which would limit how much the federal government would pay.
As described in Kansas Medicaid: A Primer 2019, states currently operate their Medicaid programs within federal standards, which include statutory and regulatory requirements as well as programmatic guidance. The amount of federal funding a state receives for Medicaid is dependent on how much a state spends on eligible services to eligible populations. The federal government matches state spending at established rates, which vary year to year based on the state’s relative economic position.
Aggregate or per-capita caps, as proposed in the HAO option, would change the federal financing structure from an established share of actual program costs to a set funding level, established either globally for the selected enrollee population (aggregate cap) or at the per-person level (per-capita cap), with limits on annual cost growth. In exchange, states could have more authority to change their programs.
Unlike some earlier block grant proposals, the HAO option is focused on adults, primarily those in the expansion population age 19-64 with household incomes up to 138 percent of the federal poverty level (FPL) who in Kansas generally are not already eligible for Medicaid.
For Kansas policymakers wondering how this could affect the current legislative process regarding Medicaid expansion, the answer can be simple or a bit more complicated.
-
- Simple version: Because it is optional to states, and because the provisions in current legislation to expand Medicaid in Kansas could be implemented without it, the HAO does not have to figure into the Kansas Medicaid expansion discussion at all.
- A bit more complicated version: Because it provides states with new programmatic flexibilities, states could consider how the HAO could be used to achieve policy goals. But they also would need to consider how the funding mechanism — either an aggregate or per-capita cap on federal spending for expansion enrollees — might affect state costs in the short- and long-term.
There is already interest in the HAO option — Oklahoma is planning to complete an application. Proponents argue that it provides states additional flexibility and establishes incentives to control costs for taxpayers. Opponents are concerned it could be used to limit coverage and benefits, and they question whether the Trump Administration can make a change of this magnitude without statutory authority, which could presage a challenge in the courts.
CMS has provided a streamlined overview of the HAO, and the Kaiser Family Foundation (KFF) has released an eight-page brief highlighting key features of, and questions about, the HAO guidance. Both are helpful resources that outline the financing requirements and policy components of the HAO, as illustrated in a graphic from the KFF brief (Figure 1).
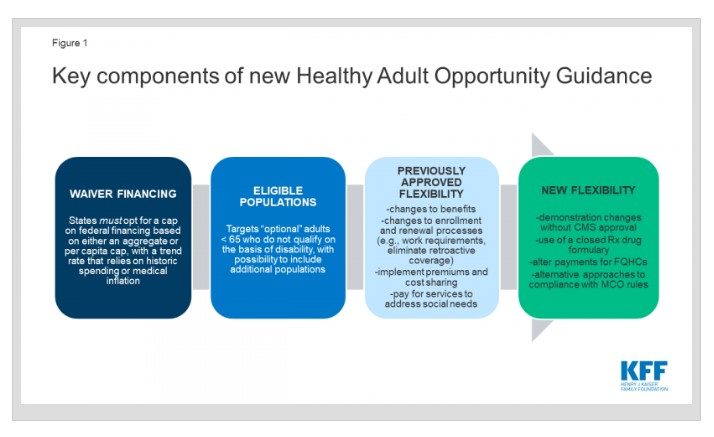
Source: Rudowitz R., Musumeci M., Garfield R., Hinton E. Implications of CMS’s New “Healthy Adult Opportunity” Demonstrations for Medicaid. Henry J. Kaiser Family Foundation. Published Feb. 5, 2020. https://www.kff.org/medicaid/issue-brief/implications-of-cmss-new-healthy-adult-opportunity-demonstrations-for-medicaid/
Elements in the HAO option familiar to those following the Kansas Medicaid expansion debate include work and community engagement requirements as well as premiums and cost-sharing above what otherwise would be allowed.
The guidance also allows for the possibility for less than a full expansion up to 138 percent FPL for adults age 19-64, but, consistent with other CMS guidance, clarifies that the federal share for any such “partial expansions” would be based on the regular Medicaid match rate (currently 59.68 percent in Kansas), not the enhanced 90 percent match allowed for an ACA expansion. Through the HAO demonstration, states may propose an alternative approach to the delivery system that “leverages the private insurance market or coverage programs designed under an applicable complementary Section 1332 waiver.”
States that opt for an HAO, which would operate under Section 1115 demonstration authority, would be able to modify administrative and programmatic components of an approved demonstration without going through a federal approval process, as long as the changes were consistent with the demonstration’s special terms and conditions. In applying for an HAO demonstration, states would need to follow the current transparency and public notice requirements of Section 1115 demonstrations.
If states select the aggregate cap funding option, they can share between 25 and 50 percent of any savings to the federal government, as long as they meet or exceed access and quality of care benchmarks. The additional federal matching funds could be used to invest in existing state-funded health programs or to provide benefits and services designed to address social determinants of health, among other options. If HAO spending exceeds its cap, the state would be responsible for the difference. The per-capita cap option does not allow for shared savings but still holds states responsible for spending that exceeds the cap.
States that want to use the HAO option to expand Medicaid would be required to start with a per-capita cap based on national data for the new adult group, adjusted for geographic factors and other information CMS deems relevant (including assumptions about pent-up demand and adverse selection). After at least two years, the state experience with the expansion group would be used to reset the baseline, and at that point the state could choose to convert to an aggregate cap.
In 2017, KHI published an analysis of how similar per-capita cap proposals in the then-GOP-controlled Congress might have affected KanCare. The 2017 simulation is useful to revisit, as it demonstrated that KanCare would have exceeded caps that were based on similar cost controls as those proposed in the HAO option. However, because the populations that would have been affected by those 2017 bills were broader than the HAO focus on “optional” adults, its findings are not perfectly applicable to the current guidance. A new model could be designed to assess the effects of an HAO demonstration. In the meantime, KHI will continue to monitor developments across the country as states weigh the HAO option.