Other Surprise Bill Protections
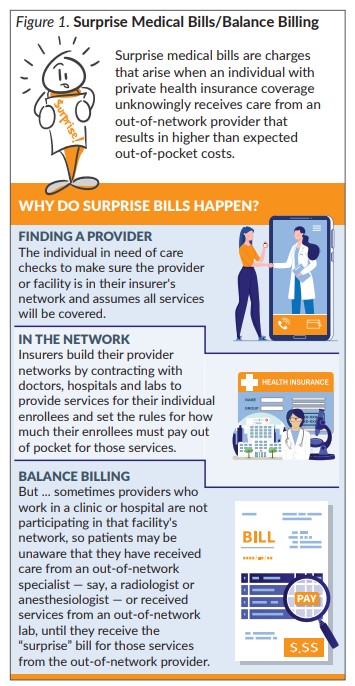
States that have enacted less comprehensive protections related to surprise medical bills have required that consumers be notified by their health plan or the hospital that they may encounter surprise bills, while others protect consumers from surprise bills associated with emergency care but not other care provided at in-network hospitals.
Kansas Legislation
During the 2020 Kansas legislative session, one comprehensive bill, Senate Bill (SB) 357, related to surprise medical bills was introduced early in the session but did not receive a hearing. SB 357 would have prohibited health insurers and health care providers from engaging in balance billing practices for services provided in hospitals, ambulatory surgery centers and provider offices, and would have made insured individuals liable only for the in-network cost sharing provided in their health plan.
The bill also prohibited health benefit plans (such as those authorized under K.S.A. 40-4602 and 40-2209), insurers and providers from issuing surprise medical bills, and required health benefit plans and insurers to pay the median in-network rate under the covered person’s health insurance to the OON provider. However, if the provider did not accept that payment, the health benefit plan, insurer or provider could negotiate an alternative amount or initiate independent dispute resolution, with certain limitations.
Federal Legislation
Most large employers self-fund health insurance for their employees. Since federal law preempts state regulation of self-funded health plans, surprise billing laws enacted by states provide no protection for consumers covered by large employers with self-funded health plans.
Federal action would be required to protect consumers enrolled in those plans. Nationally, it is estimated that over 60 percent of workers who receive coverage through their jobs are covered under self-funded health plans.
On May 9, 2019, President Trump urged Congress to enact bipartisan legislation to outlaw surprise medical bills in all types of health insurance plans. Over the last year, four House and Senate committees — House Energy and Commerce Committee; Senate Health, Education, Labor, and Pension (HELP) Committee; House Ways and Means Committee; and House Education and Labor Committee — have drafted, marked up and voted on four bipartisan bills to prevent surprise medical bills.
The three bills still under consideration would ensure that consumers do not receive surprise bills for cost-sharing beyond what they would pay for in-network providers (hold harmless protection) but differ in the way they establish what insurers will pay to OON providers. The Neal-Brady Bill (H.R. 5826), which is supported by hospitals and physician groups, provides a 30-day negotiation period, followed by independent dispute resolution if the parties do not reach an agreement. The Scott-Foxx Bill (H.R. 5800) and the Alexander-Murray Compromise Bill provide for a payment standard of the median in-network rate of the insurer for 2019 that would be inflated for future years and, for claims over $750 (or $25,000 for air ambulance cases), a binding independent dispute resolution process.
Special Protections During COVID-19
The Coronavirus Aid, Relief, and Economic Security Act (CARES Act) signed by President Trump on March 27, 2020, includes the Provider Relief Fund, which authorizes funds to be disbursed to physicians, hospitals and other providers to address the economic harm and impact on providers as a result of the pandemic. As a condition of receiving these funds, providers are required to (1) agree they will not seek to collect out-of-pocket payments from “presumptive or actual” COVID-19 patients that are more than what the patient would have paid for care from an in-network provider, and (2) are prohibited from balance billing for COVID-19 care. The CARES Act also includes language that ensures that OON lab providers will receive “fair payment” for COVID-19 testing by requiring commercial insurers to pay them an amount equal to the “cash price” for the service listed on the provider’s public website.
The Families First Coronavirus Response Act (FFCRA), signed by the President on March 18, requires “most private health plans to cover testing for the coronavirus with no cost sharing during the emergency period,” including all group health plans and individual health insurance coverage. The cost-sharing provisions do not apply to short-term health insurance policies or coverage sold by organizations like the Kansas Farm Bureau or health care sharing ministries. FFCRA sunsets on December 31, 2020.
A few states also have enacted protections for COVID-19 patients similar to those in federal law. A Connecticut executive order prohibits surprise billing for any emergency services rendered to insured patients, requires insurers to pay OON providers their in-network rate and prohibits providers from billing uninsured COVID-19 patients more than the Medicare rate for the services provided. Massachusetts has mandated in-network coverage for services related to the treatment of COVID-19, prohibited providers from balance billing consumers for the cost of OON services, and required insurers to pay OON providers the in-network rate when the insurer has an existing agreement with the hospital where the OON provider is practicing, or 135 percent of the Medicare rate if no agreement exists.
Conclusion
Although some states have taken action to protect consumers from surprise billing through state-regulated insurers, federal action would be required to protect those who are covered by large employer self-insured health plans exempt from state regulation. While the insurance industry, employers and health care providers all support legislation to protect patients from surprise medical bills, Congress is finding it difficult to balance the interests of consumers, insurers and providers when it comes to establishing how payments should be determined.