


Introduction
In March 2018, the Kansas Health Institute (KHI) released an updated estimate of Medicaid and Children’s Health Insurance Program (CHIP) enrollment if Kansas were to expand KanCare, its Medicaid program, under the terms of the Affordable Care Act (ACA).
That estimate projected that expansion would add 145,000 new beneficiaries—including 95,000 adults age 19-64 and nearly 50,000 children—to the KanCare rolls.
The projection was based on data from the American Community Survey (ACS), administered by the U.S. Census Bureau. The infographics in this fact sheet use the same data to place KHI’s projection for a Kansas expansion beside the experience in the 30 states and the District of Columbia that had expanded Medicaid on or before January 1, 2016.
Results
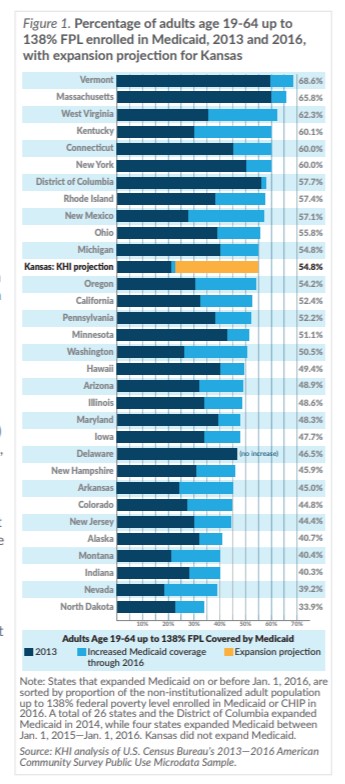
Figure 1 illustrates the percentage of adults up to 138 percent of the federal poverty level (FPL) who reported being enrolled in Medicaid in 2013, the year before the ACA’s Medicaid expansion, and 2016, the most recent year for which ACS data are available. Some states with broader adult eligibility pre-expansion had less enrollment growth after expansion than states that had more restrictive requirements to start. For example, Delaware’s 2013 income threshold was 120 percent FPL for working parents, and the state also covered childless adults. Expansion did not change the percentage of adults up to 138 percent FPL who reported having Medicaid coverage.
The Kansas bar in the chart illustrates the percentages of adults up to 138 percent FPL enrolled in 2013, 2016 and after a hypothetical expansion using KHI’s March 2018 projection. KHI’s projection would place a post-expansion Kansas below 11 and above 20 expansion states in the percentage of adults up to 138 percent FPL enrolled in Medicaid after expansion.
Kansas started in 2013 with one of the lowest percentages of adults up to 138 percent FPL enrolled, in large part because its eligibility threshold for non-disabled parents was the eighth lowest in the country, and lower than all but three states that subsequently expanded Medicaid. As a result, the projected percent increase associated with a hypothetical expansion is larger than the ACS data show for states that expanded their programs by Jan. 1, 2016.
However, expansion does not only affect enrollment for adults up to 138 percent FPL. KHI’s projection includes an estimate that nearly 50,000 children who are already eligible but not enrolled in Medicaid or CHIP would join the rolls if Medicaid were expanded.
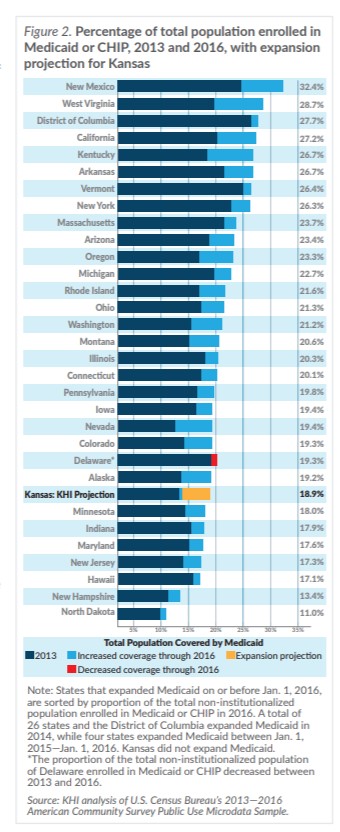
Figure 2 illustrates the percentage of a state’s entire population enrolled in Medicaid and CHIP in 2013 and 2016, and illustrates where KHI’s projection of total beneficiaries would fit within that range. In this comparison, KHI’s projection would place Kansas below 24 states and above seven in the percentage of total non-institutionalized population enrolled in Medicaid after expansion.Enrollment vs. Census Data
In part because Census data, including from the ACS, are self-reported, they may not match administrative Medicaid enrollment data reported by states. This is sometimes called the “Medicaid undercount” and is considered a function of reporting errors by survey respondents and differences in definitions between survey and administrative sources. There is significant variation among states in how closely ACS data approximate enrollment reports.
In addition, the population counts in this analysis exclude institutionalized individuals, including those residing in nursing facilities, some of whom are Medicaid beneficiaries.
Conclusion
Whether comparing only new adult enrollees or all projected enrollment growth, ACS data indicate that KHI’s projection of 145,000 new enrollees—including 95,000 new adult enrollees with income up to 138 percent of FPL—falls in the range of experience of states that expanded Medicaid.