Introduction
Suicide deaths in Kansas have increased over the past two decades, and have increased 31 percent in the last ten years alone. In 2016, suicide was the 10th leading cause of death in Kansas, and more than 500 Kansans died by suicide. This increase has occurred as other health outcomes have improved.
This issue brief describes trends and disparities that exist in suicide deaths in Kansas. It originates from the Chartbook: Racial and Ethnic Health Disparities in a Changing Kansas, which was published in December 2017 by the Kansas Health Institute (KHI). Kansas-specific data are from Kansas Information for Communities (KIC), a website managed by Kansas Department of Health and Environment (KDHE). The WONDER online databases from the Centers for Disease Control and Prevention (CDC) are used for national values.
Suicide often occurs because of a complex combination of factors including mental disorders, substance abuse and other treatable illnesses. It is included with drug overdoses and alcohol-related liver mortality in what have been called “Deaths of Despair” by some researchers.
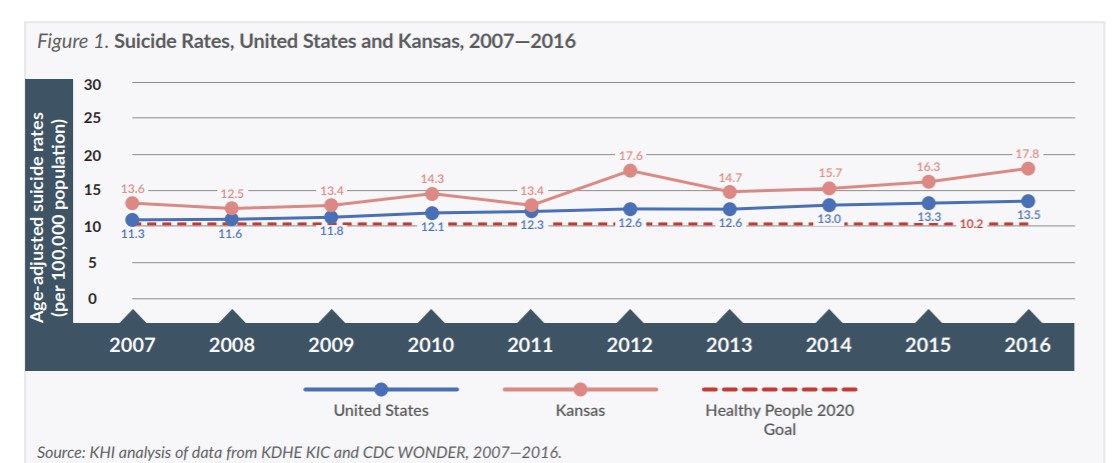
Healthy People 2020 has set a goal to decrease the suicide rate to 10.2 per 100,000 population by the year 2020. As that date approaches, the United States has moved farther away from the Healthy People 2020 goal rather than nearer (Figure 1). In 2007, the national suicide rate was 11.3 per 100,000 population; by 2016, it had increased to 13.5. The suicide rate in Kansas also fell well short of the Healthy People 2020 goal and has increased from 13.6 in 2007 to 17.8 in 2016.
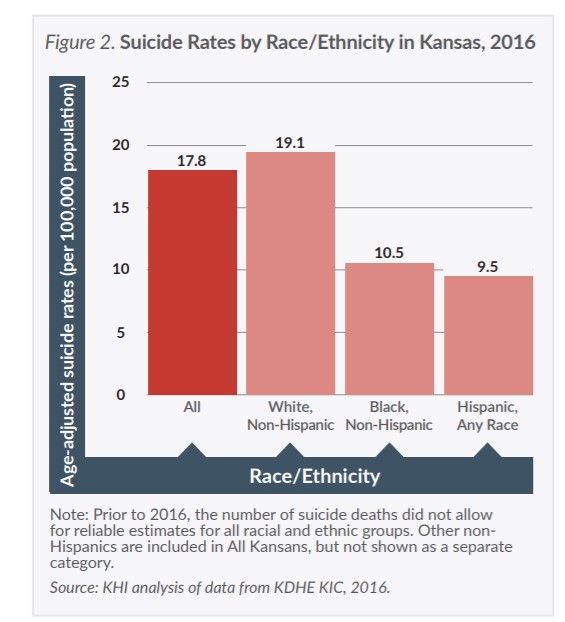
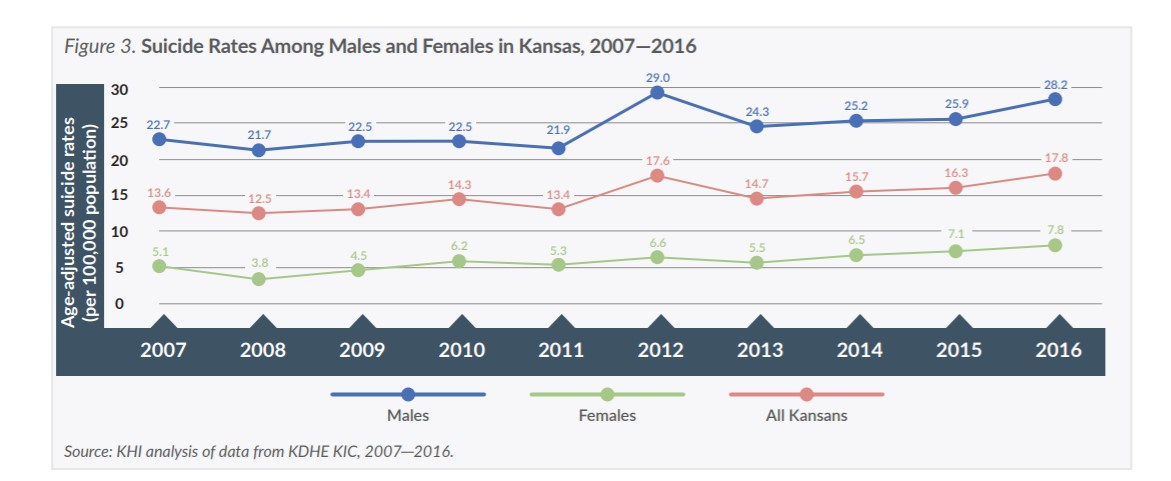
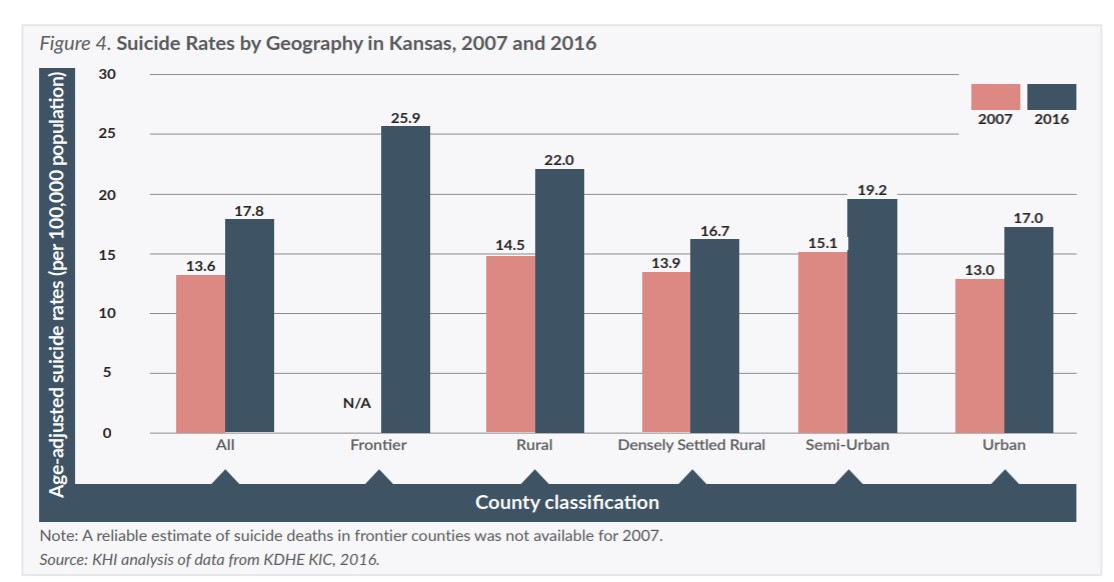
This brief focuses on disparities in suicide deaths by race/ethnicity, age, sex and geography in Kansas. Understanding disparities allows for more effective prevention to occur. When considering suicide prevention, means or method of suicide is regularly discussed. In 2016, firearms were the means for nearly half (49.8 percent) of Kansas suicides. Nationally, there are disparities in means of suicide by sub-population groups. Specifically, men and non-Hispanic Whites have the highest rates of suicide death by firearms. Other common means of death by suicide in Kansas in 2016 were suffocation (25.8 percent) and poisoning (16.0 percent). Due to small group sizes, means of suicide could not be assessed by the dimensions included in this brief (e.g., geography, age).