Risk Sharing
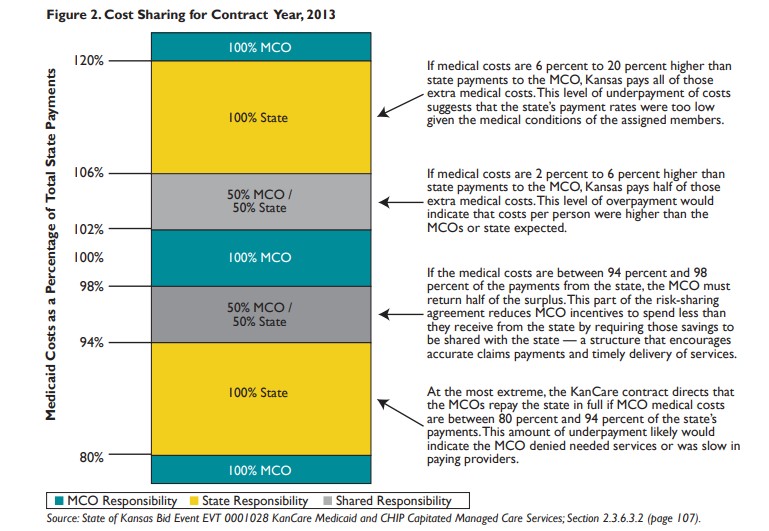
Because it is likely that an MCO will experience medical costs that will be higher or lower than the total payments from the state, the KanCare contracts include a risk-sharing requirement, shown in Figure 2. At 100 percent, MCO medical costs are equal to the state payments.
At the end of each contract year, the state will compare the MCO medical costs with the payments. Any adjustment, such as a return of funds to the state or additional state payment to the MCOs, must be made within 10 months of the end of the contract year.
Pay for Performance
One of the ways KanCare may ensure that Medicaid members receive high-quality health care is through financial incentives tied to improved health outcomes, a provision known as Pay for Performance (P4P). In KanCare, P4P withholds a portion of the state payments for release to the MCO when the contract quality terms are met. While P4P is a common mechanism to encourage quality care, there is little evidence about how P4P works when the incentives are directed to an MCO instead of health care providers.
In 2013, the first year of the KanCare contracts, the P4P withholding is 3 percent of the annual state payments. MCOs can earn this 3 percent by meeting higher performance standards for six administrative practices: timely claims processing, provider payment and service information submissions, credentialing process, grievances, appeals and customer service.
In 2014 and 2015, MCOs will have 5 percent of their state payments withheld under P4P. To earn these funds, MCOs must meet benchmarks for 15 health care quality indicators in three areas: physical health, behavioral health and long-term care. These indicators, shown in Table 1, will use each contractor’s performance in 2013 as a baseline, with increased performance required in 2014 and 2015. In addition to receiving reduced payments, contractors that fail to meet standards can be required to participate in performance improvement projects or corrective action plans.
Conclusion
Kansas has ambitious goals to improve the quality of care in its Medicaid program and reduce the rate of cost growth over time through managed care. The state’s contracts with MCOs attempt to address this balance of care and cost savings by including financial and performance guidelines as well as incentives to improve quality. Because achieving both quality and savings is an ambitious goal, it is yet to be seen how this will work in practice. However, if contractors are successful, the state may save money while also improving the Medicaid program and the health of its members.
Measure
-
- Comprehensive diabetes care
- Well-child visits in the first 15 months of life
- Preterm births
- Annual monitoring for patients on persistent medications
- Follow-up after hospitalization for mental illness
- Competitive employment for people with disabilities
- Meet benchmarks for National Outcome Measures for people with substance abuse disorders or severe mental illness
- Decreased use of inpatient services for people with mental illness
- Increased life expectancy for people with disabilities
- Increased integration of care for people with mental illness and disabilities
- Nursing facility claim denials
- Fall risk management
- Decreased hospital admissions 30 days after a nursing facility discharge
- Decreased number of nursing facility days of care
- Increased use of Promoting Excellent Alternatives in Kansas (PEAK) certified facilities
Source: KanCare Request for Proposals, Attachment J, November 2011.