Benchmark Plans Are Minimum for the Newly Eligible in Medicaid
If Kansas exercises the option to expand Medicaid coverage in 2014, Medicaid benefits will become available to all Kansans under age 65 with annual incomes at or below 138 percent of FPL, which is $32,499 or less for a family of four in 2013. Currently, adult Kansans who are not disabled or elderly or who do not have children generally are not eligible for Medicaid, regardless of their income level. The ACA requires states to provide at least a minimum set of benefits, known as the Medicaid benchmark plan, to these newly eligible people. Benchmark plans do not have to include the array of benefits available through traditional Medicaid, but some states are considering providing all Medicaid enrollees with the traditional benefit package because it may be easier to administer and better meet their health needs. Other states may choose to design their benchmark plans to cover fewer benefits and potentially avoid some costs for this newly eligible group.
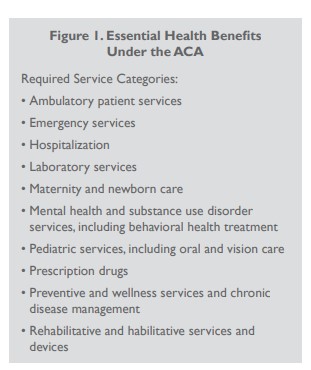
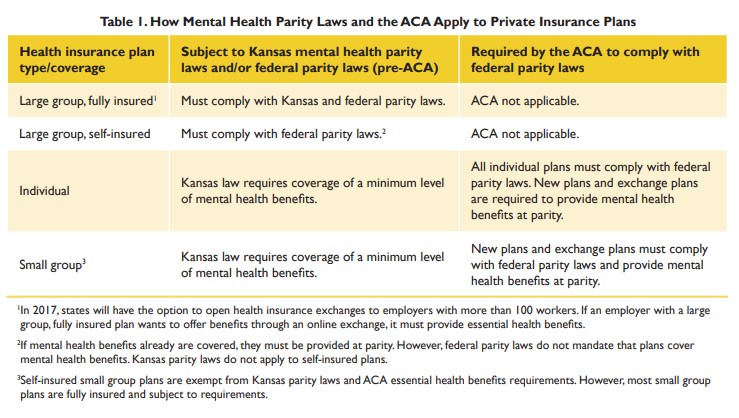
While Medicaid benchmark plans will be required to follow parity laws and cover the 10 categories of essential health benefits, including mental health and substance abuse treatment, these plans are only required to provide mental health benefits similar to private health insurance plans. Private plans, even those required to provide essential health benefits, typically do not cover community based services such as case management, peer support or attendant care offered under traditional Medicaid for Kansans with severe mental illness. Mental health research recognizes that community-based services are effective for people with severe mental illness.
In Kansas, 27 community mental health centers (CMHCs) serve people who are uninsured or underinsured, although state funding for CMHCs to serve this population has dropped about 50 percent, from $31 million in fiscal year 2007 to about $16 million in fiscal year 2013. According to the Association of Community Mental Health Centers of Kansas, just more than half of the people served by CMHCs are uninsured and about one in seven patients has private insurance. Two key state decisions — whether Kansas expands its Medicaid program to cover low-income adults and, if so, whether community-based mental health services are included in the Medicaid benchmark plan for those newly eligible enrollees — may affect the source of payment for community-based services traditionally provided by CMHCs. If community-based services are not included in the Medicaid benchmark plan, CMHCs likely will continue to depend on state funding to provide these services to the uninsured and underinsured. Additionally, if Kansas does not expand Medicaid under the ACA, as many as 130,000 low-income adults are likely to remain uninsured and many will continue to access CMHCs for mental health services. (Even with the Medicaid expansion and other elements of the ACA, experts predict a residual uninsured rate of between 4 percent and 6 percent.)
Health Homes to Coordinate Care
One of the notable mental health opportunities in the ACA is the health home option, which can be included as a component of a state’s Medicaid program. Health home services include care coordination for people with two or more chronic diseases or a chronic disease and a mental health condition.
As of November 2012, the federal government had approved health home services in eight states. Seven states have proposals under review, and 10 states — including Kansas — have been approved for planning grants. If approved for implementation, Kansas officials initially plan to pursue health homes for people with severe and persistent mental illness, diabetes or both. According to the timeline proposed for the ACA funding, these health home services would be available starting in January 2014. For a limited time, the federal government will pay an enhanced rate to the state for these services.
Missouri was awarded one of the first planning grants and began offering health home services in January 2012. Like other states, Missouri has focused on mental health, utilizing CMHCs as health home providers and mental health professionals as part of health home clinical teams. Other states, like Oregon and New York, are implementing health home options through managed care arrangements, as Kansas proposes to do. As Kansas continues to plan its health home program, state policymakers have the opportunity to seek input from mental health providers and consumers about the most effective way to coordinate care. They also can look to other states that have experimented with health home coordination for mental illness and with managed care companies.