On January 1, 2013, current Medicaid and CHIP enrollees will be automatically assigned to one of three MCOs to achieve a fair distribution of age, health needs and geographic location. They can choose another MCO within 45 days but must stay with the selected MCO for 12 months or until the next open enrollment period.
What Services are Covered?
The MCOs must provide all services currently available through Medicaid. This includes prenatal care, well-child visits, preventive services, hospital care, in-home care, community-based services and nursing facility to help enrollees with mental illness or diabetes manage their conditions. A health home model helps coordinate medical, behavioral health and social supports for enrollees. Health homes also can be used to help people with other chronic illnesses like substance abuse, asthma, heart disease and obesity.
Who Provides the Services?
MCOs must enroll providers with locations that meet access standards for covered services, including primary and specialty care, pharmacy, mental health care, emergency and long-term care. The MCOs must certify that providers are enrolled before services begin on January 1, 2013. There are financial penalties for not meeting access standards.
MCOs are encouraged to use existing resources, including hospitals, physicians, community mental health centers, safety net clinics, Centers for Independent Living, Area Agencies on Aging and Community Developmental Disability Organizations. Providers will be able to join one, two or all three MCO provider networks.
How Will This Affect Health Care Providers?
Currently in Medicaid, providers submit bills for the fee-for-service treatment they provide and receive payment from the state. With KanCare, the state will pay MCOs an amount for each person enrolled and MCOs will pay health care providers for services delivered. The MCOs must pay current Medicaid rates for each service to providers in their networks.
How Does KanCare Save Money?
KanCare is expected to reduce projected spending on the Medicaid program by $853.1 million over five years. The contract says that savings should be achieved by coordinating care and improving the health of people in Medicaid and CHIP. In their bids for the KanCare contract, the MCOs described their programs and plans to reduce the unnecessary use of medical services and improve health. Those care management tools are designed to reduce costs compared to the fee-for-service model. The per-person, per-month rate that the state negotiates with each MCO will be less than the historical cost of Medicaid.
The state also will withhold 3 percent of the MCO payments for performance incentives. In the first year of the contract, MCOs must meet six performance standards to receive the full payments. The number of performance measures and required level of performance increase in the second and third years of the contract. The MCOs must show improvement in the quality and efficiency of care or the state will keep the performance incentives.
Federal Approval Required
To implement KanCare, the state has requested a waiver from Medicaid rules from the U.S. Department of Health and Human Services. The waiver allows states to use federal funding for innovative activities or demonstration projects that would otherwise not be allowed under federal Medicaid.
States use this waiver authority for a variety of changes to Medicaid programs. Of the 34 states with approved waivers, 11 are using them to implement broader use of managed care in Medicaid as proposed in KanCare. However, Kansas’ request is more extensive because it includes more Medicaid populations and service systems and covers the whole state. Several elements of KanCare, including the mandatory enrollment of all Medicaid enrollee groups in managed care, cannot be implemented without federal approval.
Conclusion
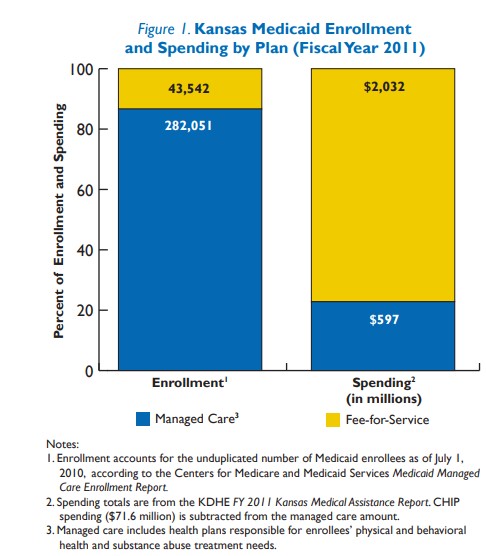
KanCare will shift more than three-fourths of Medicaid spending in the state to private managed care companies that will coordinate services. It also will introduce managed care to almost a third of Medicaid beneficiaries. The plan, subject to federal approval, has ambitious goals for achieving cost savings while significantly changing the way Medicaid services are delivered and paid for in Kansas.