Introduction
Public health is defined by three core functions: assessment, policy development and assurance. Information gleaned through assessment activities is used to guide policy development and to measure how well the public health system is fulfilling its health assurance functions.
Community health assessment (CHA) is a process of systematically collecting and analyzing data about health and health care status, issues and needs in a defined population. CHA approaches health from a broad-based perspective, taking into consideration the multiple individual, community and environmental factors that influence population health. Community health improvement planning (CHIP) utilizes results from the CHA to systematically identify and implement strategies for improving health within a community.
This brief summarizes the results of a study conducted by the Kansas Health Institute and the University of Kansas School of Medicine-Wichita in collaboration with public health practitioners across the state. The study used a mix of focus groups and surveys to gather information about CHA/CHIP experiences and outcomes in Kansas between 2012 and 2013, and finds that significant gains in practitioner confidence and progress through the CHA/CHIP process have been achieved during that period of time.
Background
In recent years, federal and state policymakers and public health organizations have placed increasing emphasis on the importance of community health assessment as a key component of effective public health. In 2010, the Public Health Accreditation Board (PHAB) issued the first set of criteria to be used in accrediting state and local health departments. Those criteria included requirements for health departments to complete community health assessments and community health improvement plans at least once every five years. The Patient Protection and Affordable Care Act of 2010 (ACA) included new requirements that tax-exempt, nonprofit hospitals conduct community health assessments at least once every three years and adopt strategies to meet the needs identified by those assessments.
Motivated by the PHAB accreditation standards and the new assessment mandate included in the ACA, many hospitals and local health departments across Kansas have embarked upon the CHA/CHIP process in recent months. For many, this was their first experience with community health assessment. Their efforts have encountered both opportunities and challenges.
Focus Group Findings
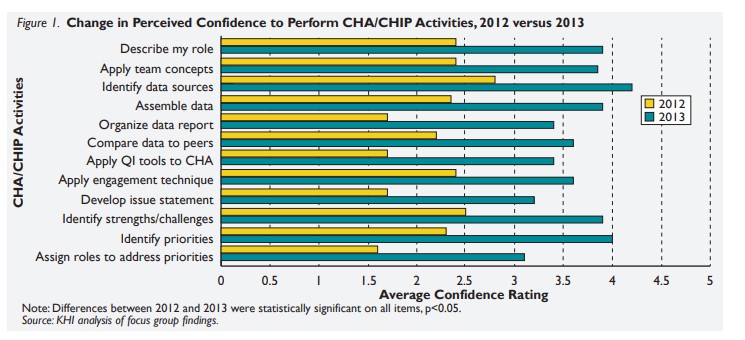
Focus groups were conducted in 2012 and 2013 with local public health/hospital representatives and stakeholders to assess opinions about inputs, processes and outcomes of CHA/CHIP activities. A brief questionnaire was administered that collected demographic information and explored participants’ confidence in their abilities to perform CHA/CHIP activities.
Focus group participants reported a number of factors that helped to facilitate CHA/CHIP progress, as well as a number of barriers. The PHAB accreditation standards and the ACA requirement were identified as motivating factors. In addition, having a history of community collaboration, strong leadership, and parallel community health initiatives were identified as factors that facilitated the process. Lack of time, competing priorities, and a need for training and technical assistance were identified as barriers that impeded CHA/CHIP progress.
At the beginning of this study, many public health At the beginning of this study, many public health practitioners were uncertain that they had the skills needed to carry out a CHA/CHIP. Rural practitioners reported lower confidence levels than those in urban areas. Between 2012 and 2013, statistically significant gains in practitioner confidence with CHA/CHIP activities were observed (Figure 1).